[printfriendly]
Clarify, def. 1. To make (an idea, statement, etc.) clear or intelligible; to be free from ambiguity. Dictionary.com
Key Points
- Create a calorie deficit
- Be aware that if you are not losing weight, you are are not creating a calorie deficit, unless…
- OCCASIONALLY, changes in water balance (typically 2-5lbs), and possibly a small gain in muscle tissue (1-5lbs) can cause the scale to mask the fact that you are actually losing fat
- Again, because it is that important, realize that if you are not losing weight, it is very likely that you are not creating a calorie deficit
Are you confused, unsure, or frustrated? These are common feelings to have when attempting to lose weight. There are a number of reasons for this. One of them stems from the bewildering amount of information about weight loss, which can seem contradictory and ultimately confusing. Most of this is due to half-truths, marketing practices, and a lack of a comprehensive, evidence-based approach to the problem. We hope to clear up some of the confusion, which should help reduce the frustration you feel. Furthermore, we hope this will result in the ability to focus on things that are worth your time, money, and effort.
The good news is, at the most basic level, the way in which the body gains or losses weight is relatively simple. You may already be familiar with the following information but it has been our experience that many people do not clearly understand some of the basic principles of weight regulation. Therefore, we felt it was necessary to include this information in an attempt to make sure everyone had a good understanding of the basics and clarify any confusion that may be surrounding this information. The goal of this chapter is to lay a solid foundation and dispel with myths about weight loss that can distract you from doing things that will likely help. Additionally, as mentioned in the first chapter, our goal is to write a book that is useful for both the public and other health professionals, so there are times when more technical aspects are covered. Feel free to skip over these parts if you want and focus on the main points. But realize that we included this information because a lack of certain details will often result in confusion and a perpetuation of false or misleading information. Finally, a number of the topics highlighted here will be explained in further detail in other chapters.re you confused, unsure, or frustrated? These are common feelings to have when attempting to lose weight. There are a number of reasons for this. One of them stems from the bewildering amount of information about weight loss, which can seem contradictory and ultimately confusing. Most of this is due to half-truths, marketing practices, and a lack of a comprehensive, evidence-based approach to the problem. We hope to clear up some of the confusion, which should help reduce the frustration you feel. Furthermore, we hope this will result in the ability to focus on things that are worth your time, money, and effort.
Sections
- A Calorie is a Measure of Energy
- Calories in One Pound of Fat (adipose tissue)
- Weight Change is Simple, in Theory at Least
- What Determines How Many Calories Your Body Burns in a Day?
- How Many Calories YOU Probably Burn a Day
- Muscle and Metabolic Rate
- Muscle and Fat Weigh the Same?
- Aging and Metabolic Rate
- But I Have a Slow Metabolism
- For Most People, Exercise Will Have Little Effect on Weight Loss
- But I Just Want to Lose Some Weight from My Midsection
- I Don’t Want to Lose Weight, I Just Want to “Get Toned”
- Water Balance
- Calorie Intake
- There are No Fattening Foods
- But I Eat Healthy
- Meal Frequency
- Eating Breakfast
- If I Just Take the Correct Supplement or Medication
- Weekly Weight Loss
- How Many Calories Should You Reduce?
- If You are Not Losing Weight it is Not Because You are in “Starvation Mode”
- You are Likely Underestimating Your Intake and Overestimating Your Activity
- Calorie Needs are Not Static
- Weight Loss: Linear or Cyclical?
- It Must Be My Genetics
- Thinking and Environmental Aspects
- I Will Just Try Harder
- I Will Just Eat Less
1 – A Calorie is a Measure of Energy
- Foods contain a certain amount of potential energy, referred to as calories.
A Calorie (kilocalorie) is a measure of the potential energy in foods and it is determined by the amount of heat necessary to raise the temperature of 1 kilogram of water 1 degree Celsius (Whitney and Rolfes 2002). This energy is derived from the macronutrient (carbohydrates, fats, proteins, and alcohol) content of the food. On an individual basis, the calorie value for each macronutrient is 4 calories, 9 calories, 4 calories and 7 calories per gram of carbohydrates, fats, proteins, and alcohol, respectively. The nutrition facts labels and the calorie content of foods compiled by the USDA are the estimations of the potential energy (calories) in the food. These are listed in books, websites (such as calorieking.com), and in “apps” such as Lose It. For example, a medium banana contains 105 calories, 1 cup of rice contains 216 calories, 4 ounces of chicken breast contains 186 calories and 1 ounce of almonds contains 168 calories.
2 – Calories in One Pound of Human Fat (adipose tissue)
- One pound of bodyfat contains about 3,500 calories.
The current estimates for the amount of calories in one pound of fat are 3,500 to 4,400 calories (Gwerder 2015). Being aware of these numbers helps to clarify how much fat a person is likely to lose per week, based on the degree of deficit that can be created. When you run the numbers to determine an estimated pace of weight loss a person can realistically achieve, the result is often one to two pounds per week. However, the numbers can be different if there is also a loss of lean (muscle) tissue, as this tissue contains about 700 calories per pound. A loss of lean tissue is common during weight loss and can represent 10 to 40 percent of the weight lost (Chaston et al 2007; Stiegler et al 2006; Weinheimer et al 2010). The range is due to a variety of variables, such as the level of calorie deficit, amount of protein intake, gender, beginning level of body fat and frequency and intensity of exercise (Chaston et al 2007; Stiegler et al 2006; Weinheimer et al 2010). A number of these variables can be modified, and if done in a certain manner, it is possible to maintain lean tissue while losing weight and therefore lose only bodyfat. However, it is pertinent to highlight the fact that during weight gain most people will gain some lean tissue and this will happen even if the person does not workout (Apolzan et al 2014; Bouchard et al 1990; Joosen & Westertep 2006). Therefore, during weight gain, there is lean tissue gain and if during dieting some lean tissue is lost it is likely that there is little to no net loss of it, relative to the amount pre-weight gain. Therefore, for most people, being overly concerned about losing a small percentage of lean tissue is unwarranted.
3 – Weight Change is Simple, in Theory at Least
- Eating more calories than the body needs and you gain weight, conversely eating fewer calories than your body needs and you lose weight.
When it comes to losing and gaining weight, it really does come down to the following basic equation;
Calories In versus Calories Out = weight gain/weight loss/ weight stabilization – let’s discuss
Weight LOSS means that Calories In is LESS THAN Calories Out

Weight GAIN means Calories In is MORE THAN Calories Out
Weight MAINTENANCE means Calories In EQUALS Calories Out

There is no quality evidence that disputes this basic premise, which is simply what the Laws of Thermodynamics would predict (Frayn 2010; Hill et al, 2012). What this means in plain English; if your goal is to lose weight you MUST create a calorie deficit. If you are not losing weight, you are not creating a deficit. Therefore, this means that you need to ingest LESS calories and/or INCREASE calories burned (i.e., increase movement; exercise duration/frequency/intensity).
4 – What Determines How Many Calories Your Body Burns in a Day?
- Your body, even at rest, will burn many calories a day, due to a number of factors.
How many calories the body will burn depends on a number of factors which are explained below. These factors determine the OUT side of the weight loss equation. The IN side (calorie intake) will be covered shortly.
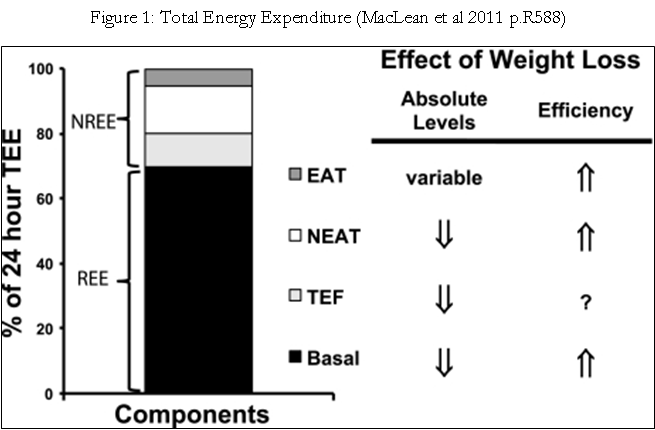
Total energy expenditure (TEE) – This represent the total amount of energy your body will burn in a day. TEE is made up of the following components; Basal metabolic rate (BMR) + Thermic effect of food (TEF) + Physical activity (PA) + Non-exercise activity thermogenesis (NEAT).
Basal metabolic rate (BMR) or resting metabolic rate (RMR): this makes about 60-80% of TEE, which means it is the main factor when it comes to how many calories you burn in a day (Shetty 2005). The only exception is if you were to exercise for at least a couple of hours a day. There is a strong genetic component to BMR and for the most part you will not be able to make any large changes to it. The following are two examples;

Thermic effect of food (TEF): This is the energy lost through heat during the digestion of different nutrients. Considering the average diet (50-60% carbohydrates, 10-15% protein and 20-30% fat) TEF is 10-15% of calories, so for 2,000 calories, the TEF will be 200 to 250 calories.(Ogata et al 2016; Whitney et al) The different macronutrients have different potential thermic effects;
- Protein: 20-30%
- Carbohydrates: 4-6%
- Fats: 1-3%
- Alcohol: 10-30%
Physical activity (PA): This includes any exercise besides the amount of movement to perform basic life functions, such as brushing your teeth, getting dressed, driving the car, etc. This also includes the walking necessary to get you to place to place. Physical activity in this sense is really any structured exercise, i.e., going for a walk or run, going to the gym, doing Pilates, etc. Regrettably, structured exercise does not burn many calories when done at a typical amount and intensity. For example, walking at a brisk pace (3.5mph) for 30 minutes will burn about 250 calories for a 250lb male and 200 calories for a 200lb female (http://www.freedieting.com/tools/calories_burned.htm). Exercise can certainly increase your TEE but to make a noticeable difference a relatively large amount of time and intensity is needed (see Exercise chapter for more details).
Non-exercise activity thermogenesis (NEAT): This is sometimes referred to as the “fidget factor”. The definition of NEAT by one researcher is “…the energy expenditure of all physical activities other than volitional sporting-like exercise” (Levine, 2007, p.275). This type of expenditure includes the amount of calories burned from shifting positions in a chair, taping your fingers or feet, occupational exercise, daily walking and stair climbing, and similar non-exercise related movements (Levine 2007; Villablanca et al 2015). Interestingly this can play a substantial role in the amount of calories burned in a day with the potential of 1,000 calories or more a day. However, for those of you who do not have a physical job, this number is likely to be more in the range of a still significant 300 calories (Levine 2007). This will be addressed a bit further in the Exercise chapter
TEE= sum [BMR + TEF + PA + NEAT]
Here is one visual (Figure 1) that will hopefully help with understanding the relative contribution of each aspect that determines TEE.
5 – How Many Calories YOU Probably Burn a Day
- How many calories a day a specific person will burn will depend on age, gender, body size, and activity levels.
As shown above, there are a number of factors that determine total energy expenditure (TEE). Since for most people, the biggest contributor of their TEE is their BMR, start by calculating this. This can be done with the formulas below or web-based calculators. The latter method is recommended, unless you enjoy doing math equations.
First, calculate your estimated BMR. There are many formulas, but the following two are likely the most accurate. Their results will likely only have about a +/- 10% margin of error (Weijs 2008) In fact, the error is more likely to be an underestimation of actual calorie needs (Prado de Oliveira et al 2011). For practical purposes, if your estimated BMR is 2,000 then it is fair to say that your BMR is in the range of 1,800 to 2,200.
If you do not know your body fat percentage, use the Mifflin-St Jeor Equation;
- Men: (10 x weight in kg) + (6.25 x height in cm) – (4.92 x age) + 5
- Women: (10 x weight in kg) + (6.25 x height in cm) – (4.92 x age) – 161
Or simply go to this website and input your numbers;
http://www.calculator.net/bmr-calculator.html
If you do have an accurate body fat percentage and therefore also have the amount of lean tissue you likely have, then use the Katch-McArdle formula; WHAT ABOUT ACTIVITY FACTORS?
- BMR = 370 + (21.6 x Lean Body Mass (kg)), this formula is for BOTH men and women
Or simply go to this website and input your numbers;
http://www.calculatorpro.com/calculator/katch-mcardle-bmr-calculator/
Then add any exercise-related calorie burn to your BMR. The following websites list many exercise/activities;
- http://www.acefitness.org/acefit/healthy_living_tools_content.aspx?id=9
- http://www.bhf.org.uk/heart-health/prevention/calorie-calculator.aspx
- http://www.healthstatus.com/calculate/cbc
Add the exercise to your BMR to get your TEE. Remember, if you are exercising only 3 days a week, you can’t add the exercise calories to the non-exercise days.
Your starting numbers: BMR= Physical activity= Total =
If you want something simpler, then the following calculator, which uses the Mifflin-St. Jeor equation and allows for a general activity multiplier, is a good choice;
There are a couple more options for determining how many calories you burn a day. The first options are the “new” personal movement devices, such as FitBit Force, Body Media Fit Core, and Jawbone UP. These devices can give you accurate reading of how much you move and exercise a day (Dannecker et al 2013; Evenson et al 2015; Stackpool et al 2015). However, your BMR is still estimated. Furthermore, for many people these can be useful tools for behavior change and behavior maintenance.
The second and most accurate option is going to get your BMR tested. These methods can tell you very precisely what your BMR is and the double label water method can tell you what your TEE is. The following methods are all referred to as indirect calorimetry.
The FitMate
- To find a place where you can get tested, go to http://www.cosmedusa.com/en/test-site-locator
The follow three types of indirect calorimetry are not easily accessible but can be available at some Hospitals and University research centers. These are all considered very accurate methods for determining metabolic rates.
- Double labeled water – the gold standard for accuracy of BMR and TEE
- Douglas Bag
- Whole room calorimetry
Recently a new portable device has come to market that can measure you metabolic rate, it’s called the Breeze. There is at least one study comparing it to a Douglas Bag and it was found to have very similar results (Xian et al 2015). Therefore, it is likely to give a person a relatively accurate measurement of BMR.
Overall, for most people, using the BMR and activity calculators will result in a fairly accurate number to work with. Again, if the numbers are not working, i.e., you are NOT losing weight, then you are not creating a calorie deficit, so decrease your intake and/or increase your physical activity. If this is hard to accept, we would strongly suggest that you find a way to get your metabolic rate (i.e., how many calories a day your body burns) objectively measured. We think this is worth the effort and expense to be able get passed this aspect.
6 – Muscle and Metabolic Rate
- Skeletal muscle tissue, think biceps, burns a small amount of calories a day, and increasing the amount of muscle is difficult. Therefore, increasing overall metabolic rate, to any meaningful amount, is unlikely for most people.
There is no doubt that the amount of skeletal muscle we have plays a role in determining our over metabolic rate or TEE. However, the fact is each pound of muscle does not burn a lot of calories a day. The evidence points to about 5-10 calories a day per pound of skeletal muscle (Heymsfield et al 2002; Ravussin et al 1986; Wolfe 2006). What this means is it is a good idea to exercise regularly (see Exercise chapter for more details) to help keep the muscle you do have. However, for many people, when they are trying to lose weight they are NOT going to gain muscle. But it is possible for some people to gain a little bit of muscle, which is in the range of 1-5lbs. Based on the calories burned per pound a gain of this much muscle could lead to an maximum increase in metabolic rate of 50 calories a day, which equates to 7 almonds. Even this is not likely because as you lose fat your metabolic rate slows down. One reason is fat tissue burns about 2 calories per pound, so lose 20 pounds of fat, which equals about 40 calories a day which leaves you with about a 10 calorie increase in metabolic rate. The point here is not to think you are going to gain a bunch of muscle and rev up your metabolism, it is very unlikely to happen. But, there are still many good reasons to exercise regularly. These benefits will be highlighter in the Exercise chapter.
7 – Muscle and Fat Weigh the SAME?
- A pound of muscle and a pound of fat are the same weight
It is amazing how many times we have heard “muscle weighs more than fat”, from clients and from other health professionals. The statement, as it is usually stated, is really nonsensical without a specific VOLUME qualifier. Here is an example; if we said “lead weighs more than feathers” then we would be making another illogical statement; does 5lbs of lead weigh more than 5lbs of feathers? I hope you said no. Obviously, 5lbs is 5lbs. However, if we said lead has a very high-density of weight and for the same amount of space lead would be much heavier, then we would be making a logical and likely obvious statement. The weight density is greater for lead than feathers; think a feather pillow versus a lead block of the same size. This is what we think people really mean when they say “muscle weighs more than fat”. They mean 5lbs of muscle is smaller than 5lbs or fat. Therefore, muscle does not weigh more than fat, again 5lbs of muscle is the same as 5lbs of fat, but rather muscle has a higher weight density. The correct statement should be “a given amount of muscle tissue will take up less space than fat tissue”. How big of a difference is there in size?
Is the weight density of skeletal muscle and fat similar to the lead versus feathers example? Hardly! It seems that the weight density difference between muscle and fat is only about 18% (http://en.wikipedia.org/wiki/Muscle). This is much less than what is typically said about the difference between these two tissues, which is usually in the range of 50 to 100%. However, this approximate 20% difference in volume could potentially make a difference in girth measurements, i.e., the size of your waist, hips, thighs, etc. This difference in waist size, etc. could occur even if you did not lose any weight. If you would to replace 5lbs of fat with 5lbs of muscle your measurements could get smaller but your weight on the scale would not change. Would you be 20% smaller? Probably not. It’s really not that simple as there are other tissues (bones in the arms and legs and organs, along with the bones from the spine for a waist measurement) that also account for the size of a specific area. The point being that the circumference of an area is not solely determined by the amount of fat and muscle and a loss of some fat and a gain of some muscle could change the size of an area, but it is likely to be a very small change. Overall, this means your girth measurements are really not going to change unless you lose bodyfat.
8 – Aging and Metabolic Rate
- As we age, our overall metabolic rate reduces a small amount per decade. However, the overall effect is rather small.
There are many statements that we have heard when someone wants to use their age as the reason they are not losing weight. A couple of examples would include “I could eat anything I wanted when I was young and not gain weight”, “Since I reached 30 or 40 or 50, I just couldn’t keep my weight down”, “It is so much harder to lose weight when you get older”, and so on. We hate to break the bad news, but the “I am older” thing does not have much of an effect on metabolic rate. In general, the research finds that a decrease in metabolic rate (BMR) per decade after the age of 20 for men is 2.9% and for women 2% (Robers and Dallal 2005). Figure 2 is a potential scenario of the decrease of BMR over the years.
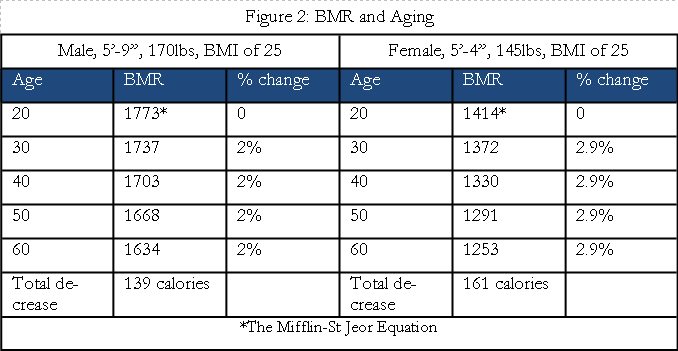
This is a real difference but it is certainly not a big difference. What is missing though is the fact that we are talking about losing weight and this means that a person has gained weight over the years. So here is a second scenario that includes a 30lb weight gain. The research has found that when people gain weight it is typically NOT all fat. The amount of the weight gain is often around 70-80% fat, meaning that there has been an increase in lean tissue (muscle, bone, etc.) of 20-30% even if you are not doing weight training or exercising at all (Apolzan et al 2014; Bouchard et al 1990; Joosen & Westertep 2006). The following scenario (Figure 3) will be conservative when it comes to the lean tissue gain and say it is 20% and the fat is 80% of the weight gained. Let’s try this again.

We feel the common views about aging and metabolism stem from hindsight bias and an unawareness of what really happens to the metabolic rate with aging. The “when I was younger I could eat anything” is probably true but not because when we are young we have a special metabolism but because it is very likely that the amount of activity or exercise a person did then was MUCH more than they have done as an adult. This could also have been due to a much higher NEAT (non-exercise activity thermogenesis), which means you could have been moving more throughout the day (this is typically not noticeable and is largely an unconscious behavior). But, the amount of calorie intake has not decreased at all or not as much as the change in the amount of calories that were burned from exercise or NEAT. This is what leads to the slow but steady increase in a persons’ weight over 10 to 20 years. For example, an extra 130 calories a day (about 2 slices of bread for example) for a year could lead to about a two pound increase in weight. A two pound increase in weight over 10 to 20 years would result in a 20 to 40 pound increase in weight (it is actually not that simple, because as you gain weight, your body will burn more calories, which would mean you would have to increase your calorie intake to keep the weight increasing). This decrease in amount of calories burned from exercise has dropped but the real change in BMR is very small. Two researcher states “Taken together, these observations indicate that BMR is indeed lower in the elderly compared with young adults even after taking body composition changes associated with aging into account, but the difference is so small…that it can be considered insignificant” (Roberts & Rosenberg, 2006, p.658). Therefore, maybe a better way to state the situation is “When I was younger I was so active that I could eat anything and not gain weight”. Overall, this not a huge effect and is generally overblown as a cause of weight struggles. One way to help reduce the small change BMR with aging is to stay active and do resistance training to help maintain the amount of skeletal muscle tissue you have (see Exercise chapter for more details).
9 – But I Have a Slow Metabolism
- Individual’s metabolisms vary, however, the range of high to low rates is rather small, and the evidence does not support the idea that a slow metabolism is the cause of most of the challenges with weight.
This is likely NOT true. We don’t mean to be so blunt. However, an abundance of evidence does not support the idea that most people who struggle with their weight have a slow metabolism (Buhl et al 1995; Carneiro et al 2016; Das et al 2004; Heymsfield et al 1995; Weinsier et al 1995). Granted, for a given set of parameters (age, gender, height, weight) there is a range of calories that will be burned. However, most people fall into a range of rates that are not significantly different, which typically means a difference of 200 calories a day. This is nothing to dismiss, but it is not like some people burn 1/2 or 1/3 of the calories of other people. The difference is likely 3 to 5% (Astrup et al 1999). For example, if the BMR of one person is 2,000 it is VERY unlikely that a person struggling with their weight will only burn 1,000 (1/2) or 1,300 (1/3) calories a day. The difference in BMR is more likely, 60-100 calories, 3 to 5% respectively. The thing is many people who swear that they have a slow metabolism don’t. When these people are tested under controlled conditions it has been clearly shown that their metabolism is right in line, given small deviations, about 3-5%, with what it should be based on their particular parameters (Astrup et al 1999; Buhl et al 1995; Heymsfield et al 1995).
Related to this aspect is the “I barely eat and can’t lose weight” statement and mindset of some people struggling with their weight. Some people state that they only eat 1,000 or less calories a day and can’t lose weight (this also includes other intakes that are not as low overall but seems to be a 1,000 or so calories less than what their estimated BMR or TEE is). This is virtually impossible. In fact, even if you were a person struggling with the awful disease of Anorexia and only weighed 96 lbs and had a BMI of 17, you would still likely lose weight on an intake of 1,000 calories. Due to the fact that many people dealing with Anorexia have spent some time in a hospital setting they have had their metabolic rates objectively tested. Here are some of the results of the metabolic rates of Anorexia patients, determined from highly accurate measures. Please take notice of the bodyweights and BMR;
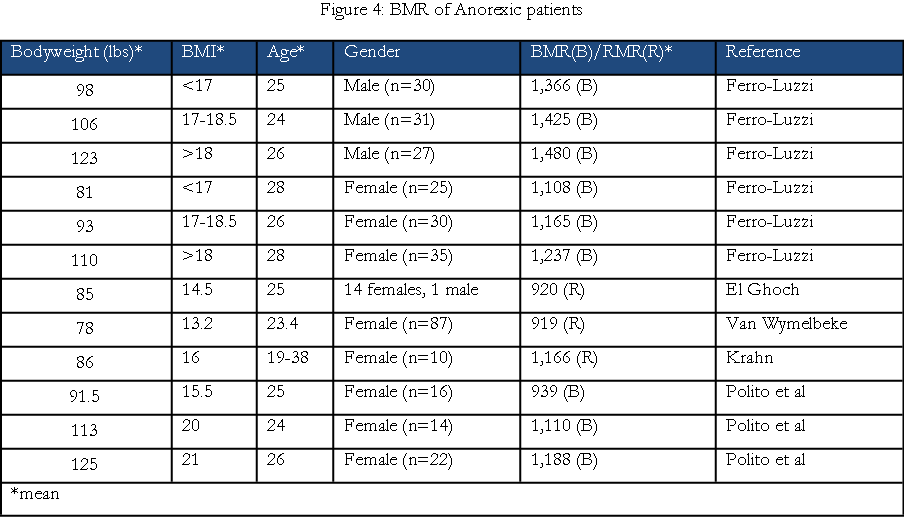
From these numbers it is obvious that even these very thin people have metabolic rates that need more than 1,000 calories to maintain their weight. Additionally, keep in mind these are the BMR numbers which means the daily total energy expenditure is higher than this, and it is safe to say that an additional 200 to 400 calories can be added to the BMR to get the TEE. For example if a person’s BMR equals 1,200, then their TEE is likely 1,400 to 1,600, respectively. Also, keep in mind that this is for someone who is not doing daily structured exercise, but rather just daily life stuff. But, you might be asking, what about people who are bigger, those that are overweight or obese. The following chart (Figure 5) highlights some of the data gathered from well-controlled and highly accurate methods for determining the BMR of normal, overweight and obese people.
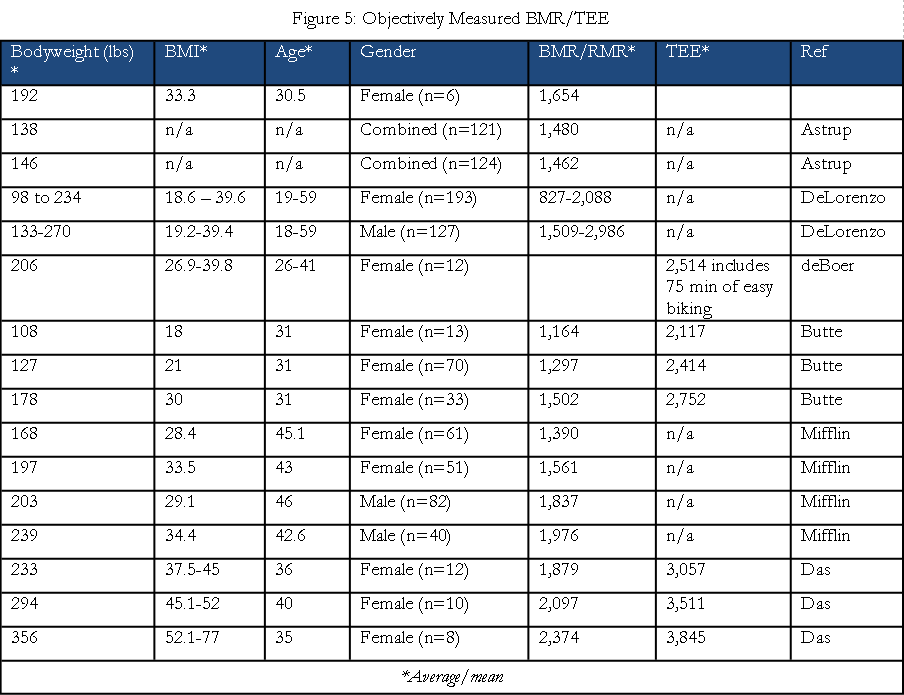
As you can see from these numbers, saying that you can’t lose weight when only eating a 1,000 calories or less a day is highly unlikely. This is not to say that eating a 1,000 calories a day is easy, it usually is not. In fact, eating fewer calories than the body needs to maintain its weight is often challenging as the body has many mechanisms in place to avoid the loss of tissue (fat). Additionally, but regrettably, for those that struggle with weight, the mechanisms for not gaining weight are often weak (MacLean et al). But, the discomfort from dieting is usually not extreme and there are methods that can help to mitigate it (see Diet, Psychology, and Exercise chapters).
If you still feel that you have a slow metabolism, there are ways to get an objective answer. There are two options. First, wearing a FitBit, Jawbone, or another movement tracker, can give a fairly accurate reading of how many calories you burn from exercise/activity in a day (Dannecker et al 2013; Evenson et al 2015; Stackpool et al 2015). The use of activity trackers is further explored in the Exercise chapter. However, this method still does not directly measure BMR and the daily TEE is an estimation based on one of the validated mathematical formulas. Therefore, the second, and best option, is going to get your BMR or TEE measured through indirect calorimetry, which as explained previously include;
- FitMate
- Breeze
- Double labeled water
- Douglas bag
- Whole room calorimetry
If you really want to get a very accurate measure of your BMR or TEE then get one of the indirect-calorimetry tests done.
10 – For Most People, Exercise Will Have Little Effect on Weight Loss
- Exercise has many physical and psychological benefits, but the amount of calories burned during exercise is often low and for most people it will have little to no effect on weight loss.
For most people, the amount of exercise they are willing and able to do will have little effect on losing weight. For example if someone was to go from NO exercise to walking 30 minutes, 5 times a week, they would increase their weekly calorie expenditure by about 450 calories (150 calories per 30 minutes). This additional calorie expenditure equates to about one-seventh of a pound of fat. Exercise has many potential health promoting benefits, but when it comes to losing weight it regrettably has little impact. Greater details on this subject will be explored in the exercise chapter.
11 – But I Just Want to Lose Some Weight from My Midsection
- Basically, you cannot force the body to lose fat from a certain area by doing specific exercises, this idea is referred to as the “spot reduction myth”.
Most people who want to lose weight want to lose the “extra” weight they are carrying in their midsection. This is a good thing, and not just for the esthetics, but due to the fact that the fat located in the midsection can largely be visceral fat, and this type of fat is the type that has negative effects on health. But, the answer to losing fat in the midsection is NOT to do crunches, side bends, wearing a belt that makes your abdominal muscle contract or wearing a neoprene type belt that makes you sweat in that area. None of these make the body “burn” the fat that is located below the muscles being worked. This belief that you can work a muscle and lose the fat that is located under it is called “spot reduction” and it is a myth. So please don’t think that you can work your “abs” and that will make you lose fat that area, it just doesn’t work that way.
12 – I Don’t Want to Lose Weight I Just Want to Get Toned
- To get “toned” you need to reduce body fat levels, which means you will lose weight.
This is a common statement when the discussion of losing weight begins and often when weight loss is not happening. This usually leads to the question; What do you mean by ‘toned’? The response is something like “more definition in my muscles, look leaner”. That is great, but, in order to get ‘toned’ you have to lose fat, which means you have to lose weight! Now to be clear, it is certainly possibly that you could gain a bit of muscle, say 5lbs, and lose 5lbs of fat, which means you would not lose weight. And yes this could get you a bit more toned. However, there are two important things to keep in mind. As explained in the ‘gaining muscle’ section, it is NOT easy to gain muscle. If you do, it is likely a few pounds over many months. Additionally, if someone wants to lose 30, 40, or more pounds, to get to a healthy weight, then getting toned means that they have to lose weight because they are definitely not going to gain that much muscle. Second, when you begin to exercise, you can get some soreness in the muscles, which is not a bad thing. This can result in a greater awareness of your muscles and this can translate into a feeling like your muscles are more toned. But, as this may feel good, it does not mean that you have lost body fat nor have you have actually gotten more ‘toned’. If someone wants to get ‘toned’, which is great, then that person has to lose weight (fat). Therefore, if you are not losing weight you are really not getting toned.
13 – Water Balance
- Due to fluctuations of water balance, our weight can vary a number of pounds over days, due to a variety of factors. This can sometimes mask some weight loss in the short-term. Conversely, it can also show a false weight gain, meaning it is not fat but water.
The body is composed of about 60-70% water, which for a 170lb male equates to about 100 pounds, and the amount is typically kept within a relatively small range, as dehydration is considered to start at a 1-2% reduction, 1 to 2 pounds, respectively and considered severe at 7 % or 7 pounds (relative to example) (Whitney and Rolfes 2002). However, it is certainly possible for people to be able to shift their weight, purposefully or not, up or down, 3 to 10lbs, due to the amount of water the body is holding. Presently there is little solid evidence of what the fluctuations will be, but the aforementioned range currently seems like a reasonable estimation. These deviations from the typical and healthy amount of fluid balance a person normally has should be short lived, a day to a week. These relatively short changes in water balance are usually due to significant acute changes in salt intake and hormonal changes such as what occurs during menstruation or high levels of stress (REF). There are typically smaller fluctuations during the day for most people due to amount of urine in the bladder, daily variations in hormones, what was eaten and so forth. This will usually translate into weighing more in the evening than the morning, which is one reason to only check your weight once a day. These are normal variations in fluid balance. However, if you are dealing with certain medical conditions, such as cardiovascular or kidney diseases, water balance is very important to monitor. Large fluctuations, which often includes significant bloating, such as pitting edema, is not a healthy situation and anyone who is dealing with this should see a healthcare professional as soon as possible. Overall, the point here is that water balance can change how much you weigh and mask the fact that you are actually losing some mass (fat and/or muscle). However, if you are trying to lose 20, 30 or more pounds, then the water fluctuation can’t hide the weight loss forever. To help deal with potential fluctuations and probably get a better understanding of your personal water balance swings, it is a good idea to weigh yourself often, preferably daily, as well as check your weight at the same time of day. Realize that big changes in diet, particularly sodium and hormonal changes can temporally affect how much water you have in your body, but if you continue to create a calorie deficit, you will lose bodyfat.
14 – Calorie Intake
- The food we eat contains calories, which come from carbohydrates, proteins, fats, and alcohol (macronutrients). The amount of calories in food and the amount that is actually absorbed is approximated. The amounts can give us a good idea about how much we are ingesting, but it is not exact or perfect.
The IN part of the equation is the calories ingested from food and drinks. Calories are really a measure of potential energy. When it comes to food there are four energy yielding nutrients (macronutrients), which are;
- Carbohydrates: 4 calories per gram
- Proteins: 4 calories per gram
- Fats: 9 calories per gram
- Alcohol: 7 calories per gram
As mentioned earlier the different macronutrients have different TEF (thermic effects of food) potentials. This means that the actual amount of calories (energy) remaining after metabolizing the different nutrients will be different. However, the differences, although real, often do not lead to any real world difference. The potential exception is protein. If you exchange some fats and carbohydrates with proteins, and ingest a relatively high protein diet (see Diet chapter for more details) then it is possible for you to increase your metabolic rate (TEE) by about 50 calories a day.
Additional aspects, which can potentially reduce the accuracy of the estimation of how many calories you are eating, are the Nutrition Facts labels. These are not always exact and be off the mark enough to make the totals for the day be off by hundreds of calories.
One final thing regarding this aspect; the potential calorie amount for a given food is just that, it’s potential. The food has to be digested and absorbed into the blood stream in order for the potential energy to be available. This means that variations in digestive efficiency can modify the amount of calories that are actually liberated from food. This means the actual amount of calories absorbed from the food could be less than the label. Therefore, the amount of calories you are getting from your food will likely varying from the amount that is listed on the nutrition facts label. Changes in digestive efficiency can play a small in role weight loss. Regrettably, there is not much you can do about it. But knowing this, you can realize that if you are not losing weight you will need to decrease your overall calorie intake to continue your weight loss.
15 – There are NO Fattening Foods Only Fattening Quantities
- Calories, more specifically excess calories, are fattening. No food will automatically cause fat gain, regardless of what it is made of. Only excess calories, from any food (broccoli or brownies), will cause weight gain or inhibit weight loss.
We don’t know how many times we have heard the statement “I can’t eat that, it’s fattening”. This “fattening food” label has been placed on many items. Usually if you ask why it is fattening, the response will refer to a particular nutrient in the food, such as “It’s high in sugar”, or “It’s high in fat”. This can also refer to a variety of other reasons such as “it’s processed”, “it’s digested quickly”, “it has artificial sweeteners in it”, and so on. Now all of these things may be true, but it does not make a food inherently fattening. Here is the reason, a food can ONLY be fattening IF you eat an amount that is MORE (by itself or leads to more calories overall) than the amount of calories you burn in a day. For example, if you eat 2 donuts for breakfast (336 calories), a regular soda for a snack (136 calories), PB and Jelly sandwich on white bread (382 calories) and I packet of Ramen noodles for dinner (385 calories) which amounts to about 1,300 calories for the day and if this 1,300 calories is less than the amount of calories you burn in a day, which it likely is, you will lose weight. This is hardly a healthy diet, but that is a different subject. We are talking about calories and if your calorie intake is less than you burn, regardless of where the calories come from, you will lose weight. Interestingly, Mark Haub, a nutrition professor at Kansas State University, did follow a diet, referred to as the Twinkie Diet, that was filled with processed foods (about two-thirds of the diet was made up of junk foods) and lost 27lbs in 10 weeks along with significant improvements in his cholesterol and triglyceride levels (Parks). To be clear, we are NOT suggesting this is a good way to eat on consistent basis. However, this lends more weight to the fact that calories are king. This means you CAN eat any food, including ones that are typically on the naughty list (depends, of course which diet book you are reading), such as almonds (all nuts), avocados, butter, pasta, rice, grains, even the gluten containing ones, and practically anything at a Fast Food restaurant and so forth and still LOSE weight. The main point here is that there are NO fattening foods, there are only fattening quantities of food. There are some nuances to this and other related aspects that will be explained in greater detail in the Diet chapter.
16 – But I Eat Healthy
- All foods contain calories, regardless of their real or perceived health status. Eating healthier will not always means you are eating fewer calories.
It is a good thing, for your overall health, that you are focusing on eating healthy. However, eating healthy does not mean you will automatically eat fewer calories. In fact, the belief that eating healthy or adding something healthy to a meal will make it more effective for weight loss has been coined the ‘dieters paradox’ (Chernev 2010). If have been focusing on eating more whole foods keep doing that. But, if you are not losing weight, it means you are eating too many calories and it doesn’t matter that those calories are coming from healthy foods. In fact, a couple of review papers related to this topic came to similar conclusions (Kaiser et al; Mytton et al). One of the papers; Increased fruit and vegetable intake has no discernable effect on weight loss: a systematic review and meta-analysis, concluded, as you could guess from the title,
“Studies to date do not support the proposition that recommendations to increase F[fruit]/V[vegetable] intake or the home delivery or provisions of F/Vs will cause weight loss. On the basis of the current evidence, recommending increased F/V consumption to treat or prevent obesity without explicitly combining this approach with efforts to reduce intake of other energy sources is unwarranted” (Kaiser, et al. p.567).
This does not mean more fruits and vegetables should not be eaten. In fact, based on the research regarding the effects of low calorie dense foods on appetite, generally having the ability to make you feel full on fewer calories, this can still be an important part of your success (Ellon-Martin et al 2005; Karl et al 2014). But, when it comes to losing weight, you still have to consider the overall calorie intake.
Additionally, as stated in the “there are no fattening foods” section, eating what can be considered less healthy or unhealthy foods, does not inhibit weight loss as long as calorie intake is at the correct level.
17 – Meal Frequency
- It doesn’t matter
Eating the same amount of calories, but with different frequencies, (i.e, many small meals, say 6, versus 2 or 3 relatively larger meals), has NO effect on daily (24 hour) metabolic rate. Therefore, when it comes to losing weight meal frequency will not change the amount of weight that will be lost.
18 – Eating Breakfast
- It doesn’t matter.
Related to the meal frequency aspect, when you start your eating has no effect on your overall metabolic rate. Therefore, eating breakfast does not stimulate metabolism and a person will not burn more calories for the day because something was eaten soon after rising.
19 – If I Just Take the Correct Supplement or Medication
- A few supplements may have a small effect and the current medications for weight loss can have a small to modest effect on weight loss. However, at this time, the effects are short-term, can be expensive, and really do not address many of the aspects that determine eating and exercise behaviors that are required for long-term success.
We wish we could say that there is an over-the-counter (OTC) supplement or a prescription medication that can have a significant impact on losing weight, but that is currently not the situation. When it comes to OTC supplements, for the few that have actually been shown to work, the amount of additional weight loss caused by the supplement is very small, such as 1-2 pounds a month. Tkhe 1-2 pounds comes as an added expense of forty or more dollars, resulting in about 20 dollars per pound of weight loss. Moreover, keep in mind, the vast majority of weight loss supplements do NOT elicit any additional weight loss. This topic will be covered in great detail in the Supplement/Medication chapter. Additionally, at the time of this writing, the website Examine.com is an outstanding resource for evidence-based information about weight loss supplement and supplements in general.
When it comes to weight loss medications, there are currently nine of them (Mayo Clinic 2015). They all work, meaning they can help with weight loss. These medications will typically cause a greater amount of weight loss than the few OTC supplements that actually work. The most recent evidence suggest that they can lead to while using the medication a loss of 7 to 20 pounds can occur (Wharton et al 2015). Furthermore, realize that this amount of weight loss usually occurs over one year. This is potentially a clinically meaningful amount of weight loss. However, there are concerns about side effects from long-term use as well as maintenance of the weight loss when the medication is discontinued (Yanovski et al 2014). Like all interventions, it is really about what amount of weight can be kept off that matters. Additionally, typically when there are positive results from using these drugs they are used along with dietary and exercise interventions.
The main concern or point regarding the use of both OTC and prescription medications for weight loss is the fact that they do not address many of the factors that influence both short-term and long-term weight loss. These products may be helpful and can be part of a comprehensive and effective approach. But by themselves, they will often have a small impact overall, so thinking or hoping that they can be the answer to weight challenges can lead to false hope and a lack of focus on what can actually help with the situation. This will be discussed in detail in the Supplement and Medication chapters.
20 – Weekly Weight Loss
- For most people, consistently losing 1-2 pounds a week is realistic.
All of this information has really been about how to lose weight (fat). In order for your body to metabolize stored energy, i.e., fat (adipose tissue) there needs to be a deficit between how many calories are coming in and how many are going out. To facilitate the loss of one pound of fat you will need to have caused the body to burn off about 3,500 calories of stored energy (fat). To be clear, one pound of human bodyfat contains at least 3,500 calories. To get to the 3,500 calorie deficit you need to have a daily deficit of about 500 calories (7 x 500 = 3,500). This would lead to a weight loss of one pound. Increase the deficit to 1,000 calories a day (7 x 1,000 =7,000) and you lose about two pounds. The following chart (Figure 6) displays what that could look like.

Based on these numbers it is easy to see where the general recommendation to “lose 1 to 2 lbs a week” comes from. For this example, the TEE is not very big so this rule is very fitting. We added the 1,500-calorie deficit to illustrate that 3 pounds a week is possible, but that only leaves about 500 calories to eat for the day. This is generally not a good strategy to follow for long periods of time, maybe a week or two. But what about people how have a much higher TEE? What about people who seem to lose 5 – 10 pounds in a week? First, these high amounts are typically not ongoing and only happen for a week or two due to water fluctuations (reduced muscle and liver glycogen, due to following a low carb diet and/or high levels of exercise and low overall calorie intake, which leads to less overall water content). Additionally these people tend to be very big and they are exercising a lot. The following chart (Figure 7) displays what that this can look like.
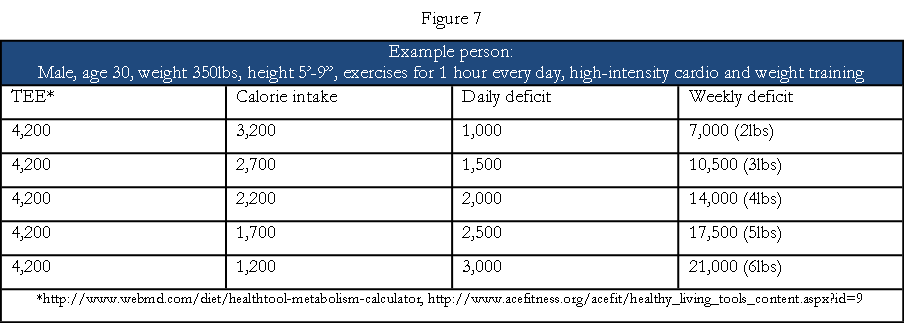
As you can see from this scenario, it is certainly possible for a large person, who exercises daily, to lose up to six pounds a week, of fat, and still be able to eat about 1,000 calories a day. Doing 2, 3 or 4 hours of exercise a day can certainly increase this number to 8 to 10 pounds a week. This is what happens on the weight loss shows, but back to reality. A bigger person can certainly lose 3-5 lbs a week, if they exercise daily, and still be able to eat 2,700 to 1,700 calories a day, respectively. Even for the big person who does not exercise, losing 3-4 lbs a week is not impossible as this would necessitate a daily intake of about 1,600 to 1,100 calories, respectively. Therefore, the amount of weekly weight loss will depend on how big you are, how much exercise you do, and what level of calorie intake you can consistently maintain. Three major caveats: First, losing weight without exercise is likely to lead to a far greater amount of muscle loss (see Exercise chapter for more details). Furthermore, calorie intakes in the lower range, which can facilitate a more rapid weight loss, will often not have enough room to get the proper amount of protein, which contributes to the greater muscle loss (see Nutrition chapter for more details). Second, these examples have all been based on losing ONLY fat. Regrettably there will often be some loss of muscle tissue while losing weight, but not always (see Exercise and Nutrition chapters). The fact is muscle only has about 700 calories per pound (REF). Therefore, losing some muscle along the way to your goal weight can skew the numbers a bit. For example, (Figure 8) using the 80% fat and 20% lean tissue ratio used above regarding weight gain, the numbers would be this;
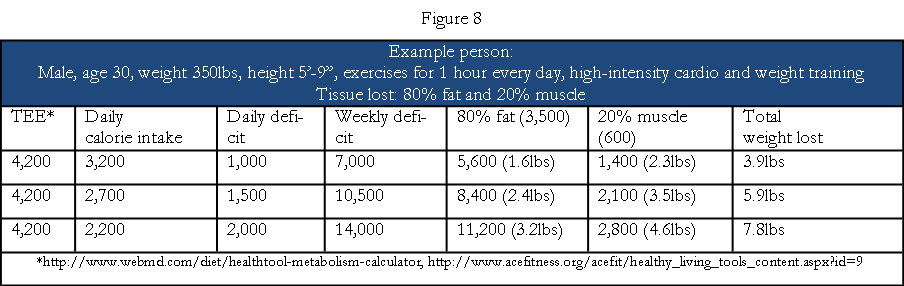
These amounts of muscle loss are not likely to occur. This was purely an example to highlight the calorie differences between fat and muscle tissue. A more likely result during weight loss would be;
- With a 20lb weight loss OVERALL there would be a loss of about 4lbs of muscle (20%)
Third, the 3,500-calorie rule is not an exact number and recent research has pointed out that this general premise has some limitations and can often lead to an overestimation of the amount of weight a person will lose (Hall et al, 2012). Therefore, realize that the numbers many not add up and deviations from the estimates are likely to occur and it is probably safe to say that the real world results will be less than the estimated weight loss from a given calorie intake.
Overall, this should give you a good understanding of what a realistic amount of weight loss that can occur weekly based on your particular parameters and behaviors.
21 – How Many Calories Should You Reduce?
- About 500 to 1,500 less than maintenance intake
As stated above there are a number of factors that contribute to TEE (total energy expenditure) and therefore how many calories you need to ingest to facilitate weight loss. It is likely that small changes in calorie intake, 100-200 calories is too small of a goal. Two reasons for not using such a small change in intake; first it is very hard to calculate your typical calorie intake with such precision that you can likely modify intake of such a small amount. Second, there is the real possibly that such a small change in calorie intake will be compensated with a change in NEAT, which could easily cancel out the decrease and result in no calorie deficit. A decrease of daily calorie intake in the range of 500 to 1,500 calories is probably a safe bet. But, again, if you are not losing weight then you are not causing a calorie deficit, so no matter what amount you think you are eating and/or moving, you need to change them to continue to lose weight.
22 – If You are Not Losing Weight it is NOT Because You are in Starvation Mode
- Eating a low amount of calories, or no calories, will not inhibit weight loss.
There is a meme that eating too little calories will actually inhibit weight loss. This concept is usually referred to as the “starvation mode”. The following is a good definition of the “starvation mode”, written by Jay while writing an excellent article on the subject;
To lose weight, you need to consume less calories. BUT, if you consume TOO few calories, your metabolism slows down so much so that your body enters a state where weight loss stops completely.
Some people also believe being in this state of not eating enough calories not only prevents weight loss from happening, but it can also cause weight gain.
So basically, eating too little prevents your body from losing weight. In some cases, it might even cause it to gain weight. To get “out” of this state and start losing, you must eat more calories, not less.
This, according to most people, is what starvation mode is. (Retrieved from http://www.aworkoutroutine.com/starvation-mode/)
This is a somewhat common view given by the lay public to try to explain a lack of weight loss when there seems to be very little calories eaten. Regrettably, this is also a fairly common reason given by “professionals”. For example Dr. Peeke on WebMD had this to say in a post titled “Stop Starving Yourself”;
Although you may think it makes sense, eating very little over the long term does not help you shed pounds. Instead, it actually teaches your body how to hold onto your weight. You see, the body is hardwired to do whatever it takes to help you survive. When you drastically cut your calories, you will drop some weight. However, if you keep doing that, the body adapts and adjusts to what it considers to be life threatening starvation. Your body does not know whether you’re on a desert island with nothing to eat, or you’re sitting in an office in Manhattan deliberately starving yourself. It’s all the same to your biology. The end result is that the body becomes very efficient at burning the fuel it has (your fat) and eventually you’re not burning much at all and thus the thwarted efforts to drop weight. (retrieved from http://blogs.webmd.com/pamela-peeke-md/2009/07/stop-starving-yourselves.html)
Dr. Peeke is implying that eating a low amount of calories will inhibit weight loss. There are changes to metabolic rate when calories are restricted, this will be further explained below, but to say that eating few calories, which will result in a the body going into starvation mode, resulting in your body “not burning much at all and thus thwarted efforts to drop weight” is false. In reality there is NO “starvation mode” as typically presented, such as the definition given by Jay. What this means is, your body cannot inhibit weight loss if you are eating less calories than your body burns. EVERYONE who eats a low amount of calories, which will cause a calorie deficit, will ALWAYS loss weight and this has been demonstrated repeatedly in a variety of experiments. Not to mention all the horrible starving that has been purposefully done to certain groups of people throughout history which always lead to significant weight loss. Additionally, all of the people who struggle with Anorexia lose considerable amounts of weight, with BMIs usually below 16, sometimes as low as 12 (e.g. a weight of only 70lbs at height of 5 feet 4 inches) and the concern is always that they have lost too much weight from eating very little (El Ghoch et al 2012; Van Wymelbeke et al 2004). There are also the people who have purposefully gone on a hunger strike to protest or bring awareness to a cause.
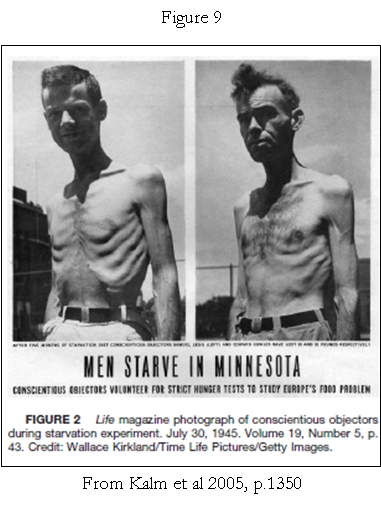
The following are just a few examples from the research done over the past 60 years demonstrating that there is no “starvation mode”. First, in 1944 a group of young men, 36 of them at first and ending with 34, volunteered to participate in the Minnesota Starvation Experiment, which consisted of a weight loss phase that lasted 6 months and produced approximately a 25% reducing in weight during that time (Kalm et al 2005). This was not a fast, but rather a restricted calorie diet, with daily intakes during the weight loss phase, of 1,800 calories. This intake varied some based on the weight loss progress, as the goal was to elicit about 1kg (2.2 lbs) of weight loss per week. The tables (Figures 10 and 11) from the original work published by Keys and colleagues shows that ALL participants lost a considerable amount of weight during the 6 months. The following picture (Figure 9) helps to clarify what starvation looks like.

The above charts (Figures 10 and 11) data is not very clear, as this is a copy of a document from 1945. Therefore, we made a chart (Figure 12) that clearly shows the amount of weight loss for each participant.
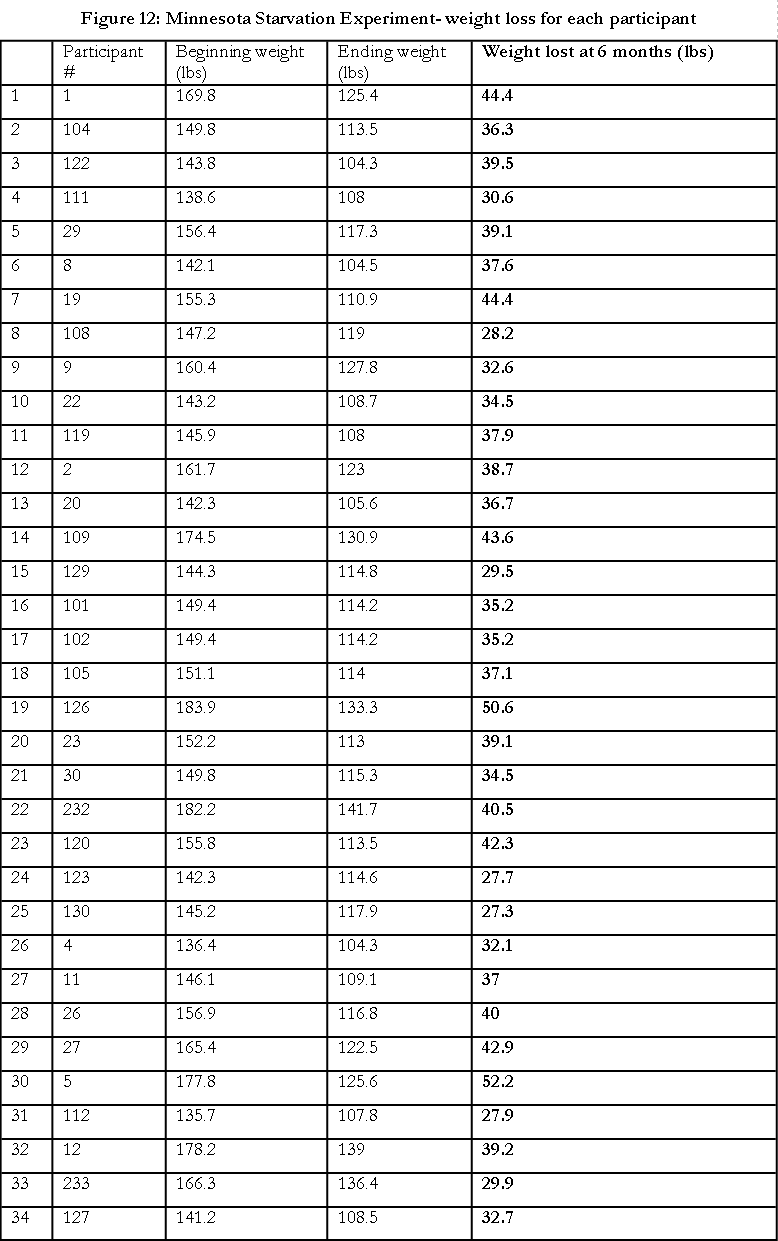
As you can see, ALL of the participants lost a considerable amount of weight during the 6 months with an average weight loss during the 6 months of 37 pounds. Keep in mind that these men were already lean when they started the diet. Their average starting BMI was 23.
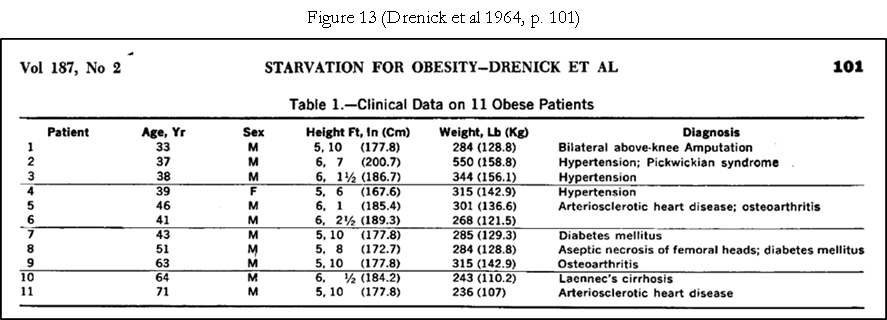
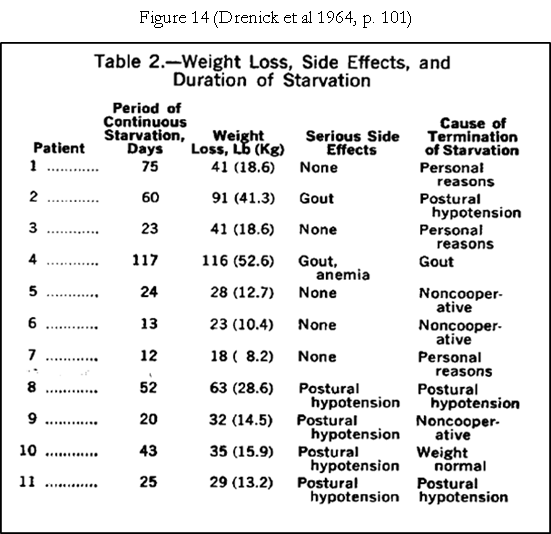
The next study is another oldie but goodie. This paper, titled Prolonged Starvation as Treatment for Severe Obesity, was published in JAMA in 1964. In this study 11 obese (10 males and 1 female) individuals were hospitalized on a metabolic-balance ward from 12 to 117 days and only given as much water as they wanted and a few vitamin and mineral supplements (Drenick et al 1964). What happened? Did they not lose weight because they went into “starvation mode”? Absolutely not! The amount of weight loss ranged from 18 lbs (12 days) to 116 lbs (117 days), with an average weight loss of .91 pounds a DAY, nearly a pound a day. The following two tables (Figures 13 and 14) from the paper clearly show the beginning metrics and the amount of weight loss for each individual.
The next study looked at the weight loss of 14 pairs of obese female identical twins. This was another metabolic ward study, with the participants staying in inpatient units for 40 days with 28 days of a weight reduction phase. All food and activity was closely monitored. The following table (Figure 15) from the paper gives some of the important bio-metric outcomes (Hainer, V. et al 2001).

During the weight loss phase (28 days) the participants ingested only about 382 calories a day. Additionally they did daily exercise, which was a 4km walk, 20 minutes on a stationary bike and 30 minutes of aerobic exercise. What was the result? The mean weight loss was 8.8 kg (19.4 lbs), with a range of 5.9kg (13 lbs) to 12.4 kg (27.3 lbs). Using the mean weight loss of 19.4 lbs, the average weight loss per week was 4.85 lbs. The point here is all the participants lost weight, a significant amount, even though they were only eating about 382 calories a day.
The next tightly controlled study involved 5 patients who were scheduled for Roux-en Y gastric bypass surgery (Huerta, S. et al. 2009). These 5 patients were hospitalized for an average of 10.6 weeks (8 to 15 weeks). The diet consisted of a liquid calorie diet which amounted to 891 calories and 83.7 grams of protein. The 5 patients also did some water-based exercise once or twice a week for 30 minutes. A few specifics about the patients before telling you how much weight they lost. These patients, all males, were all morbidly obese, with an average BMI of 64 and a corresponding average bodyweight of 468.8 lbs. This is important to consider when looking at the amount of weight they lost. The average weight loss during the dietary intervention was 85.8 lbs (range of 62 to 102lbs) resulting in an average weight loss per week of 8lbs. Again, a low amount of calorie intake led to a substantial amount of weight loss and certainly did not inhibit weight loss.
The next study is a very recent one. This one entailed a 50% reduction in calorie intake from maintenance level, for 6 weeks. This was a metabolic ward type study so food intake, as well as activity levels, were tightly controlled and monitored. Below (Figure 16) are the results for the 12 participants;
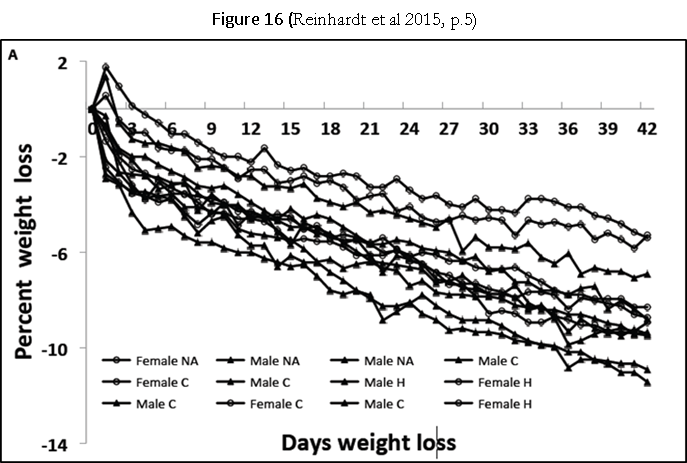
Again, as you can see EVERYONE lost weight when calorie intake was reduced 50%. However, the amount of weight loss (% of weight) was not the same for everyone. This variation is likely due to genetic differences, referred to as the thrifty-phenotype (Reinhardt et al 2015). To be clear, having the thrifty-phenotype will not inhibit weight loss, but rather will make it more difficult to lose weight as well as keep the weight off.
We will wrap this section up with two more studies about two individuals fasting. The first one is actually a 44 day fasted completed by David Blaine the illusionist (Jackson, J. et al 2006). This was a complete fast, which meant the participant only ingested water. This was done in London, in complete public view and was video-taped, during the entire 44 days (https://en.wikipedia.org/?title=David_Blaine, https://en.wikipedia.org/?title=David_Blaine#/media/File:Dbatbday.jpg). When the 44 days ended Mr Blaine had lost 53.9 lbs, going from 211.2 lbs (BMI of 28.4) to 157.3 lbs (BMI of 21.3) (Jackson, J et al, 2006). Again, no “starvation mode” occurred even though he at no food, and, in fact, he was starving.
{kind=link}
The final example that should clearly drive home this point; in 1972 a 27 year old man weighing 456lbs started a medically supervised fast which lasted 382 days. Yup, the young man fasted for 1 year, 2 weeks, and 4 days. This was a true fast, meaning there were no calories ingested and only non-calorie beverages and a few vitamin and mineral supplements, which were prescribed. During this time he lost 276lbs, which means he averaged a 5lb lose a week. The young man was able to maintain his daily life during this time and the authors of the paper stated “Prolonged fasting in this patient had no ill-effects” (Stewart et al, p.203). You must be thinking; He must of gained it all back. Five years after stopping the fast he has been able to maintain his weight at 196lbs, meaning he was able to keep off 260 of the 276lbs he lost.
To be clear, we are NOT recommending anyone fast for this long unless under medical supervision. The point is eating NO calories would be the epitome of starving, and if it actually inhibit weight loss, this is when it would definitely do it. Yet, this young man, and others who eat nothing, or very little, ALL lose a considerable amount of weight. Yes, there is a real thing called starving and it is not a good thing. But, eating a low amount of calories, (say 1,000), when you have 30, 40, or more pounds of extra body fat is not really the same thing as eating only a few hundred calories a day when you ALREADY have a low amount of body fat and have to endure this for long periods of time. Whenever you eat fewer calories than your body needs to maintain its current weight, it will fairly quickly respond in a way that will try to minimize the loss but NOT inhibit it. This reaction by the body is called adaptive thermogenesis. When you eat less calories than the amount that maintains your current weight, which is EVERY diet that elicits weight loss, the body has the ability to adjust it’s BMR and TEE and/or the amount we will move per day (possible changes in NEAT) and the metabolic (i.e., caloric) response to exercise, which, again, is known as adaptive thermogenesis (AT). How much and how quickly this adaptation occurs depends on the amount of calorie reduction, activity levels, frequency of the deficit, and genetics (Heymsfield et al; MacLEan et al; Major, et al). There is almost always some AT when a deficit between calories in and calories out, i.e, a calorie deficit, occurs. But, this AT can only adjust so much, and that is why the body cannot inhibit weight loss if calories are low enough. The body HAS to use a certain amount of energy (calories) to run no matter how low a calorie intake is.
Another good article on the subject by Dorene Robinson RD, CDN, states this about the starvation response because of a large decrease in calorie intake;
Metabolic rates don’t actually drop enough to significantly slow weight loss (if someone is indeed adhering to a reduced-calorie target). There can be a small reduction in (resting) metabolic rate when you reduce your calorie intake. For most people—since they’re eating 1,200 or more calories per day—that drop won’t be more than 5%. For the minority of people that eat fewer calories (which should only occur under medical supervision) the reduction may be 5- to 15%.[i] In neither case will weight loss STOP, or stall, beyond what’s explainable by those changes. Under no circumstances will EATING MORE be necessary. Not everyone will experience this reduction in metabolism, but for those that do it dissipates a week or so after they resume a calorie intake level that matches (or exceeds) the physiolgical needs of their current body weight.[ii] (retrieved from http://www.beyonddiets.com/beyonddiets-blog/2012/3/9/starvation-mode-fact-or-fiction.htmla )
The idea that eating too little calories will stop weight loss is not true. Most people will agree with this if they take a minute and think about it. We hope at this point the previous information has clearly shown that the “starvation mode” as a reason for not losing weight has no merit. So please do not blame a lack of weight loss on this fictitious “starvation mode” response. With all that said, there are calorie intakes as well as macronutrient intakes (protein especially) that is likely easier to maintain and will likely reduce the amount of muscle that might be lost. Additionally, very low calorie intakes and very fast weight loss, does have other potential negative health effects. Therefore, even though low calorie intakes will not inhibit weight loss it certainly may not be a good option when it comes to certain health aspects. For more details on these subjects see the Nutrition chapter.
23 – You are Likely Underestimating Your Intake and Overestimating Your Activity
- Many people eat more than they think they do and move less than they think they do.
The evidence is clear that many people do a poor job reporting how many calories they actually intake. Often the reported intake is 30 to 50% less than actual intake (Buhl et al 1995; Lichtman et al 1992; Novotny et al 2003; Stice et al 2015). This will translate into being off by 500 to 1,000 calories of actual intake. Additionally, people will often overestimate the amount of activity or exercise they do, which can mean overall calorie expenditure is a couple hundred calories less than expected (Atienza et al 2005). There are a number of psychological reasons for this as well as the fact that it can be difficult to know how much of a food you are actually eating (Maurer et al 2006; Novotny et al 2003; Tooze et al 2004). Additionally, active dieting and being overweight, is associated with more underreporting (Novotny et al 2003; Stice et al 2015). The point is, if you are not losing weight and your food diary states that you are ingesting a certain amount of calories that is very likely to elicit weight loss then it is very likely you are ingesting more calories as well as moving less than you think you are.
24 – Calorie Needs are NOT Static
- There is no exact, constant calorie intake needed daily for weight loss.
The amount of calories your body needs will usually vary slightly on a day-to-day basis. Your calorie needs will also change when you lose weight. Additionally, changes in physical activity will also change your calorie needs. This means a calorie intake that may have worked in the past to lose weight will not work forever and adjustments of intakes will be needed to continue losing weight.
25 – Weight Loss: Linear or Cyclical?
- Losing weight in phases or a linear path are both viable options.
You have decided to lose weight and have cut calorie intake and increased your activity levels, excellent! But, once you start can you never take a break from eating less? We didn’t mention stopping exercise because there are so many physical and psychological benefits derived from regular exercise that it really should be separated from “weight loss”, .i.e, “I exercise to lose weight” should be replaced with “I exercise because I feel better, physically and mentally, and it helps me burn a few more calories a day” (see Exercise chapter for more details). Anyways, does weight loss have to be linear; point A to point B process? The short answer, NO. There is no evidence that people who lose weight weekly or strive to lose weight weekly are better off in the long run than people who oscillate between times of purposefully striving to lose weight and purposefully striving to maintain their weight. At this time there is no best method for losing the weight and keeping it off. Therefore, you need to find out what works for your particular needs. But, there is enough research supporting some type of cyclical method that is should be an option (Alhamdan et al 2016; Granttan Jr, B. et al; Rossner; Varady; Williams et al). We think having the option to be able to oscillate between periods of greater focus and drive to lose weight and a more relaxed state of maintenance will help to eliminate or at least reduce the “all or nothing” thinking, such as the “I am on a diet and can’t stop until I reach my goal weight”. Additionally, as important it is to lose the weight, the most important part is maintaining the new weight. This is the part that can last, hopefully, 30, 40, or more years and the time it took you to get to your desired weight is likely only 6 months to 2 years. Based on those numbers, it would seem that practicing maintaining your weight could only help (see The Long Haul chapter for more details about maintaining your new weight). Here is one example (Figure 17) to illustrate a cyclical method to losing weight over 1 month;
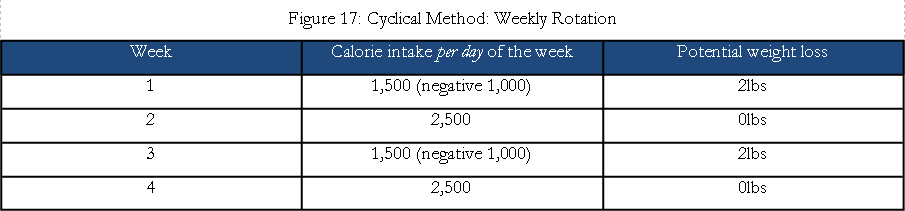
The result of this scenario would be a 4lb weight loss in four weeks but only had to “diet” for two weeks. Intermittent fasting is another cyclical method that can work well for some people (see Nutrition chapter for more details).
26 – It Must Be My Genetics
- Like all conditions, genetics play a role, however, for nearly all of the people who struggle with their weight, their genetics are not really the cause.
The quick answer is no. This is a somewhat flippant answer. We mean no, with respect to how most people seem to being trying to use “genetics” as a reason they cannot lose weight. Essentially, for almost all people who struggle with their weight, it is not due to a gene, or multiple genes that causes them to gain weight or inhibit weight loss. However, there is much more to this topic (see information in the chapter What is a healthy weight?). Briefly, like most diseases (obesity is currently defined as a disease by the AMA and other groups, but this is currently a contentious issue), there is an interaction of genetics and environment, the nature and nurture, respectively, concept (O’Rourke 2014). There are genetic predispositions that make it easier for many people (about 60% of the US population is classified as overweight or obese) to create a calorie surplus and gain weight (Choquet et al 2011; Chung et al 2008; Farooqi et al 2006). Conversely, these same people will have genetic predispositions that make it harder to create a calorie deficit, particularly consistently. Therefore, they have difficulty in losing weight. More specifically there can be differences in hormones that regulate metabolism and appetite, as well as reward sensitivity, stemming from differences in dopamine and other neurotransmitters that affect behavior, just to name a couple of things. Overall, it is clear that for many people their genetics makes it easier to gain weight (which entails frequently creating a calorie surplus), and conversely more difficult to lose weight, in an obesogenetic environment (however, everyone on a deserted island with little food will lose weight, but it is clear this is not a realistic option except for the few people who go on reality shows such as Survivor). The genetics and weight aspect has been referred to as “Genes load the gun, the environment pulls the trigger” (Bray 2004, p.115). For most people, there are strategies (environmental and cognitive) to mitigate these challenges, which are controllable and result in the ability to reach and maintain a healthy weight (Heshmat 2011; Jansen et al 2015; Riekert et al 2014). Many parts of this book will address these strategies.
27 – Thinking and Environmental Aspects
- How we think, and our surroundings, play a major role in our eating and exercise behaviors.
We have covered some of the physiological aspects of weight management, highlighting some of the basic aspects that matter and a number of things that don’t matter. But, before concluding, we want to quickly highlight the fact that there are psychological and social aspects that are very important. In fact, these aspects can often be more important when it comes to being successful, i.e, being able to consistently do the things that lead to reaching and maintaining a healthy weight. These aspects will be explored in detail in their respective chapters, for now just a few highlights.
28 – I Will Just Try Harder
- Effort is needed, but it must be used properly.
As much as we appreciate the idea and willingness to put forth more effort, this is often not the reason for a lack of progress. To be clear, there are times when there is a lack of effort (physical or mental). But, underlying this lack of effort is often a lack of motivation, particularly the intrinsic type and determination/resilience, which often stems from a lack of meeting some core psychological needs and a lack of congruence with what is considered really important for an individual. This will manifest as low willpower or effort. But the remedy is usually not saying “I will just do it” or “I will try harder”. These statements may result in an acute spike in motivation, but they will not change the psychological barriers that are getting in the way of ongoing adherence. Additionally, there are many drivers of behavior that are occurring outside of conscious awareness which are the social and environmental settings that a behavior is going to take place in. This means that at decision points, such as what am I going to choose on the menu, how much of this am I going to eat, will I get on the treadmill when I get home, and others, there are learned beliefs, attitudes, and the environmental context (surroundings) that can strongly drive what we will done at any single moment. Therefore, just saying you will try harder which often manifests as “I am just going to do it” (sorry Nike, it usually is not that simple) often does not actually lead to you doing it, particularly long-term. With that in mind, it is often not about working harder, and telling yourself you just have to do it and being pumped up, but rather working smarter. Working smarter can mean approaching the challenge in a different way, often by utilizing strategies that can change how you relate to the situation as well as changing the environmental components that will strongly influence behavior. The Psychology and Environment chapters will go into detail about this.
29 – I Will Just Eat Less
- Saying it and doing it is often not the same thing.
Yes, this is one of the things that must happen for weight loss to occur. However, saying one is going to eat less and actually eating less is often not the same thing. Therefore, there usually needs to be the use of specific tools, such as journaling food intake (self-monitoring) as well as measuring foods (Burke et al. 2011). Furthermore, having an eating plan can also help with this. In addition, changing environmental aspects, such as what foods are in the house, size of bowls and plates and so on. The point is there typically needs to be the use of conscious deliberate strategies if someone is going to eat less on a consistent basis. Therefore, thinking that eating less will just happen, intuitively, is unlikely to happen.
In Conclusion
Weight loss is rather simple but is often difficult to do. The goal of this chapter was to clarify some of the basic aspects of losing weight. We hope that this allows you to devote more time to implementing evidence-based strategies, such as those found throughout this book, that will help you reach your healthy weight and most importantly be able to stay at that weight, give or take a few pounds.
References
Alhamdan, B.A. et al (2016). Alternate-day versus daily energy restriction diets: which is more effective for weight loss? A systematic review and meta-analysis. Obesity Science & Practice; 2(3): 293-302.
Apolzan, J. et al (2014). Effects of weight gain induced by controlled overfeeding on physical activity. American Journal of Physiology – Endocrinology and Metabolism; 307(11): E1030–E1037
Astrup, A. et al (1999). Meta-analysis of resting metabolic rate in formerly obese subjects. Am J Clin Nutr; 69: 1117-1122.
Atienza, A. & King, A. (2005). Comparing self-reported versus objectively measured physical activity behavior: a preliminary investigation of older Filipino American women. Research Quarterly Exercise Sport; 76(3): 358-362.
Bouchard, C. et al (1990). The Response to Long-Term Overfeeding in Identical Twins. NEJM; 322:1477-1482
Bray, G. A. (2004). The epidemic of obesity and changes in food intake: the Fluoride Hypothesis. Physiol Behavior; 82: 115-121.
Buhl, K. et al (1995). Unexplained disturbances in body weight regulation: Diagnostic outcome assessed by doubly labeled water and body composition analysis in obese patients reporting low energy intakes. J Am Diet Assoc; 95: 1393-1400.
Butte, N. (2003). Energy requirements of women of reproductive age. Am J Clin Nutr; 77: 630-638.
Carneiro, I. P., Elliott, S. A., Siervo, M., Padwal, R., Bertoli, S., Battezzati, A., & Prado, C. M. (2016). Is Obesity Associated with Altered Energy Expenditure? Advances in Nutrition, 7(3), 476–487. http://doi.org/10.3945/an.115.008755
Chaston, TB. et al (2007). Changes in fat free mass during significant weight loss: a systematic review. Inter J Obesity; 31: 743-750.
Chernev, A. (2010). The dieter’s paradox. J Consumer Psychology. 21: 178-183.
Choquet, H. & Meyre, D. (2011). Genetics of obesity: what have we learned? Current Genomics; 12: 169-179.
Chung, W. & Leibel, R. (2008). Considerations regarding the genetics of obesity. Obesity; 16(supple 3): S33-S39.
Dannecker, KL. et al (2013). A comparison of energy expenditure estimation of several physical activity monitors. Med Sci Sports Exerc.; 45(11):2105-12. doi: 10.1249/MSS.0b013e318299d2eb.
Das, S.K. et al (2004). Energy expenditure is very high in extremely obese women. J Nutr; 134: 1412-1416.
De Boer, J. et al (1986). Adaptation of energy metabolism of overweight women to low-energy intake, studied with whole-body calorimeters. Am J Clin Nutr; 44: 585-595.
De Lorenzo, A. et al (2001). Measured and predicted resting metabolic rate in Italian males and females, aged 18-59y. European J Clin Nutr; 55: 208-214.
Drenick, E. et al (1964). Prolonged starvation as treatment for severe obesity. JAMA, 187(2): 100-105.
El Ghoch, M. et al (2012). Resting energy expenditure in Anorexia Nervosa: measured versus estimated. J Nutrition and Metabolism; 652932.
Ello-Martin, J. et al (2005). The influence of food portion size and energy density on energy intake: implications for weight management. Am J Clin Nutr; 82(suppl): 236S-241S.
Evenson, KR. et al (2015). Systematic review of the validity and reliability of consumer-wearable activity trackers. Int J Behav Nutr Phys Act.; 12:159. doi: 10.1186/s12966-015-0314-1.
Farooqi, S. & O’Rahilly, S. (2006). Genetics of obesity in humans. Endocrine Reviews; 27(7): 710-718.
Ferro-Luzi . et al (1997). Basal metabolism of weight stable chronically undernourished men and women: lack of metabolic adaption and ethic differences. Am J Clin Nutr; 66: 1086-1093.
Frayn, K. (2010). Metabolic Regulation. A Human Perspective (3rd Ed). Wiley-Blackwell. West Sussex, United Kingdom
Grattan Jr, B. et al (2012). Addressing weight loss recidivism: A clinical focus on metabolic rate and the psychological aspects of obesity. Int J Obesity; 56753.
Gwerder, Nicholas Samuel (2015). A theoretical analysis examining the construct of a pound of fat equaling 3,500 kilocalories. Retrieved from https://csus-dspace.calstate.edu/handle/10211.3/139453
Hainer, V. et al (2001). A twin study of weight loss and metabolic efficiency. Inter J Obesity, 25: 533-537.
Harvie, M. et al (2011). The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: a randomized trial in young overweight women. Int J Obesity; 35(5): 714-727.
Heshmat, S. (2011). Eating Behavior and Obesity. Springer, New York.
Heymsfield, S. et al (1995). The calorie: myth, measurement, and reality. Am J Clin Nutr; 62 (suppl): 1034s-1041s.
Heymsfield, S. et al (2002). Body-size dependence of resting energy expenditure can be attributed to nonenergetic homogeneity of fat-free mass. Am J Physiol Endocrinol Metab; 282: E132-E138.
Hill, J. et al (2012). Energy balance and obesity. Circulation; 126: 126-132.
Huerta, S. et al (2009). Feasibility of a supervised inpatient low-calorie diet program for massive weight loss prior to RYGB in superobese patients. Obes Surg;
Jackson, J. et al (2006). Macro- and micronutrient losses and nutritional status resulting from 44 days of total fasting on a non-obese man. Nutrition; 22: 889-897.
Jansen, A. et al ((2015). A cognitive profillf obesity and its translation into new interventions. Frontiers in Psychology; 6: 1807.
Joosen, A. & Westertep, K. (2006). Energy expenditure during overfeeding. Nutrition & Metabolism; 3:25 doi:10.1186/1743-7075-3-25
Kaiseer, K. et al (2014). Increased fruit and vegetable intake has no discernable effect on weight loss: a systematic review and meta-analysis. Am J Clin Nutr; 100: 567-576.
Kalm, L. & Semba, R. (2005). They starved so that others be better fed: Remembering Ancel Keys and the Minnesota Experiment. J Nutrition; 135: 1347-1352.
Karl, JP. & Roberts, SB. (2014). Energy density, energy intake, and body weight regulation in adults. Adv Nutr.; 5(6):835-50. doi: 10.3945/an.114.007112.
Keys, Ancel, et al (1945). Experimental starvation in man. University of Minnesota.
Krahn, D. et al (1993). Changes in resting energy expenditure and body composition in anorexia nervosa patients during refeeding. J Am Diet Assoc; 93:434-438.
Levine, J.A. (2007). Nonexercise activity thermogenesis – liberating the life-force. J Internal Med; 262: 273-287.
Lichtman, S. et al (1992). Discrepancy between self-reported and actual calorie intake and exercise in obese subjects. N Engl J Med; 327: 1893-1898.
Maurer, J. et al (2006). The psychosocial and behavioral characteristics related to energy misreporting. Nutrition Reviews; 64(2): 53-66.
Mayo Clinic (2015). Common weight-loss drugs. Retrieved from http://www.mayoclinic.org/healthy-lifestyle/weight-loss/in-depth/weight-loss-drugs/art-20044832?pg=2
McLean, P. et al (2011). Biology’s response to dieting: the impetus for weight regain. Am J Physiol Regul Integr Comp Physol; 30: R581-R600.
Mifflin, M. et al (1990). A new predictive equation for resting energy expenditure in healthy individuals. Am J CLin Nutr; 51: 241-247.
Mytton, O. et al (2014). Systematic review and meta-analysis of the effect of increased vegetable and fruit consumption on body weight and energy intake. BMC Public Health: 14:886
Nieman, D. et al (2006). Validation of Cosmed’s Fitmate in measuring oxygen consumption and estimating resting metabolic rate. Research Sports Medicine; 14: 1-8.
Novotny, J. et al (2003). Personality characteristics as predictors of underreporting of energy intake on 24-hour dietary recall interviews. J Am Diet Assoc; 103: 1146-1151.
O’Rourke, R. (2014). Metabolic thrift and the genetic basis of human obesity. Ann Surg; 259(4): 642-648.
Ogata H, et al (2016). A novel approach to calculating the thermic effect of food in a metabolic chamber. Physiol Rep;4(4). pii: e12717. doi: 10.14814/phy2.12717.
Park, M. (2010). Twinkie diets helps nutrition professor lose 27 pounds. Retrieved from http://www.cnn.com/2010/HEALTH/11/08/twinkie.diet.professor/index.html?hpt=T2
Prado de Oliveira, E. et al (2011). Comparison of predictive equations for resting energy expenditure in overweight and obese adults. J Obesity; doi:10.1155/2011/534714
Ravussin, E. et al (1986). Determinants of 24-hour energy expenditure in man. J Clinical Investigations; 78: 1568-1578.
Reinhardt, M. et al (2015). A Human Thrifty Phenotype Associated With Less Weight Loss During Caloric Restriction. Diabetes; doi: 10.2337/db14-1881
Riekert, K. et al (2014). The Handbook of Behavior Change (4th Ed). Springer. New York
Roberts, S. & Dallal, G. (2005). Energy requirements and aging. Public Health Nutrition; 8(7): 1028-1036.
Roberts, S. & Rosenberg, I. (2006). Nutrition and aging: Changes in the regulation of energy metabolism with aging. Physiol Rev; 86: 651-667.
Sameul-Hodge, C. et al (2004). A comparison of self-reported energy intake with total energy expenditure estimated by accelerometer and basal metabolic rate in African-American women with type 2 diabetes. Diabetes Care; 27: 663-669.
Schoeller, D. (2009). The energy balance equation: looking back and looking forward are two very different views. Nutrition Reviews; 67(5): 249-254.
Shetty, P. (2005). Energy requirements of adults. Public Health Nutrition; 8(7a): 994-1009.
Stackpool C. et al (2015). ACE-SPONSORED RESEARCH: ARE ACTIVITY TRACKERS ACCURATE? Retrieved from https://www.acefitness.org/prosourcearticle/5216/ace-sponsored-research-are-activity-trackers
Stewart, W.K. & Fleming, L.W. (1973). Features of a successful therapeutic fast of 382 days’ duration. Postgraduate Medical J; 49: 203-209.
Stice, E. et al (2015). Elevated BMI and male sex are associated with greater underreporting of calorie intake as assessed by doubly labeled water. J Nutrtion; 145: 2412-2418.
Stiegler, P. & Cunliffe, A. (2006). The role of diet and exercise for the maintenance of fat free mass and resting metabolic rate during weight loss. Sports Med; 36(3): 239-262.
Tooze, J. et al (2004). Psychosocail predictors of energy underreporting in a large doubly labeled water study. Am J Clin Nutr; 79: 795-804.
Van Wymelbeke, V. et al (2004). Factors associated with the increase in resting energy expenditure during refeeding in malnourished anorexia nervosa patients. Am J Clin Nutr; 80: 1469-1477.
Varady, K.A. (2011). Intermittent versus daily calorie restriction: which diet regimen is more effective for weight loss? Obesity Reviews; 12: e593-e601.
Villablanca, P. et al (2015). Nonexercise activity thermogenesis of obesity management. Mayo Clinic Proc; 90(4): 509-519.
Weijs, P. (2008). Validity of predictive equations for resting energy expenditure in US and Dutch overweight and obese class I and II adults aged 18-65 y. Am J Clin Nutr; 88: 959-970.
Weinheimer, E. et al (2010). A systematic review of the separate and combined effects of energy restriction and exercise on fat free mass in middle aged and older adults: implications for sarcopenic obesity. Nutr Reviews; 68(7): 375-388.
Weinsier RL, Nelson KM, Hensrud DD, Darnell BE, Hunter GR, Schutz Y.(1995). Metabolic predictors of obesity. Contribution of resting energy expenditure, thermic effect of food, and fuel utilization to four-year weight gain of post-obese and never-obese women. J Clin Invest.;95(3):980-5.
Wharton, S. & Serodio, K.J. (2015). Next generation of weight management medications: implications for diabetes and CVD risk. Curr Cardiol Rep; 17(5): 35.
Whitney, E. & Rolfes, S. (2002). Understanding Nutrition (9th Ed). Wadsworth. Belmont, CA.
Williams, K. et al (1998). The effect of short periods of caloric restriction on weight loss and glycemic control in type 2 diabetics. Diabetes Care; 21(1): 2-8.
Wolfe,R. (2006). The underappreciated role of muscle in health and disease. Am J Clin Nutr; 84:475–82.
Xian X, Quach A, Bridgeman D, Tsow F, Forzani E, et al. (2015) Personalized Indirect Calorimeter for Energy Expenditure (EE) Measurement. Glob J Obes Diabetes Metab Syndr; 2(1): 004-008. DOI: 10.17352/2455-8583.000007
Yanovski, S. & Yanovski, J. (2014). Long-term drug treatment for obesity: A systematic review and clinical review. JAMA; 311(1): 74-86.
[printfriendly]