Insulin levels do NOT directly affect the ability to lose fat in overweight, obese, unhealthy, or older humans.
Insulin being THE hormone that determines what happens with weight is popular lately, due to the resurgence of the Keto diet. Is insulin THE hormone? No! Directly connected to this is carbohydrate intake as this is the macronutrient that elicits insulin release (protein does as well but often to a lesser degree). Higher insulin levels or insulin resistance as well as higher carbohydrate intakes (this is an ill-defined concept, but for now it will be referred to as higher than 40% of calories) do not directly cause fat gain nor do they directly inhibit fat loss. People can lose all the fat they want even if they are eating a high amount of carbohydrates (they don’t have to but they can). Furthermore, high carb intakes do not elicit negative metabolic changes when in a hypocaloric state, in fact, there is almost always improvements in important metabolic markers (such as fasting glucose, insulin sensitivity, cholesterol, inflammation, etc). These should not be a controversial statements, particularly in 2019. Regrettably, due to things said by many people who promote low carb diets, which includes Keto, as “THE” diet, these ideas still seem pervasive. These incorrect ideas about insulin and carbohydrates is really a red herring and it can frequently lead people to focus on the wrong things. Losing weight and maintaining a healthy weight is already challenging, let’s not make it harder for no good reason.
The following will highlight some of the key studies and review papers on the topic of insulin levels as well as carbohydrate intake and its effects on fat loss that have been done over the past 20 years. These will be in chronological order and not necessarily in order of importance.
The Research (well just some of it, but enough that should make a clear and well-supported point)
1996-Similar weight loss with low or high-carbohydrate. Am J Clin Nutr; 63(2):174-8.
“The results of this study showed that it was energy intake [calories], not nutrient composition, that determined weight loss in response to low-energy diets over a short time period.” (emphasis added)
Some key aspects of the study
- N=43
- Age/Gender:
- Low carb group (A), mean Age 41, 3 males and 19 females
- High carb group (B), mean Age 45, 6 male and 15 female
- BMI:
- (A), mean of 41.3
- (B), mean of 38.6
- Diets:
- (A),15% carbs, 32% protein, and 53% fat
- (B), 45% carbs, 29% protein, and 26% fat
- both at 1,000 calories a day, food was distributed over 3 meals and one snack
- This was a metabolic ward study, meaning all participants lived in the hospital for the entire intervention and were very closely monitored daily and all food was provided to participants
- Exercise- consisted of 1 h of aerobic exercise training per day and 1 h of underwater physical activity per day.
- Intervention was 6 weeks
- Weight loss– Group A=17.6 lbs, Group B 15.4 lbs
- Eating a wide range of macronutrients, while in a calorie deficit, lead to a clinically significant amount of weight loss and eating a diet of 45% carbs clearly did not inhibit fat loss (15.4 lbs in 6 weeks)
1998-Metabolic and behavioral effects of a high-sucrose diet during weight loss. Am J Clin Nutr; 65(4): 908-915.
“Results show that a high sucrose [40% of calories] content in a hypoenergetic, low-fat diet did not adversely affect weight loss, metabolism, plasma lipids, or emotional affect.”
Some key aspects of the study
- N=42 (all females)
- BMI: mean of 35.93
- Age: mean of 40.3
- Diet: 2 diets, a high (43%) and a low (4%) sucrose diet, HS and LS respectively, but both had the same overall macronutrient intakes of 71% carbs, 19% protein, and 11% fats.
- To be clear, the high sucrose diet had 43% of total calories coming from sucrose (table sugar)
- Duration: 6 weeks
- Weight loss: HS = 15.3 lbs, LS = 16.2 lbs, over 2lbs per week, with a total carb intake at 71% of calories and one of the diets containing 43% of total calories as sugar.

1999-Differences in insulin resistance do not predict weight loss in response to hypocaloric diets in healthy obese women. J Clin Endocrinol Metab.;84(2):578-81.
“It is concluded that the ability to lose weight on a calorie-restricted diet over a short time period does not vary in obese, healthy women as a function of insulin resistance or hyperinsulinemia.”
Some key aspects of the study
- N=31 (all female)
- BMI: mean of 31
- Age: mean of 43
- Diet: goal of a daily 1,000 calorie deficit, which was from a commercial liquid nutrition formula (shake) and 2 high fiber muffins and a sodium supplement.
- Weight loss over 8 weeks was a mean of 24lbs
1999-THE HAWAII DIET: Ad libitum high carbohydrate, low fat multi-cultural diet for the reduction of chronic disease risk factors: obesity, hypertension, hypercholesterolemia, and hyperglycemia. Hawaii Medical Journal; 7: 69-73
“The high carbohydrate. low fat, low energy density, multi—ethnic Hawaii Diet administered ad libitum was demonstrated to induce a significant weight loss and a reduction in systolic hypertension, total cholesterol. LDL. and serum glucose.”
Some key aspects of the study
- N=22
- Gender: 10 males/12 females
- Age: mean of 49.9
- BMI: mean of 35.6
- Medical conditions: 6 with hypertension, 4 with diabetes with one of them taking insulin, 2 with glucose intolerance and one with hypothyroidism taking synthroid
- Intervention was 21 days
- Diet: very high carb diet, 77% carbs, 12% protein and 11% fats, all food was provided
- There was a daily morning check-in at testing facility
- Weight loss: mean of 10.3 lbs, (range of 5 to 33lbs), mean of 6.4% of starting BW
- So a very high carb intake did not inhibit fat loss
2005-Effect of high protein vs high carbohydrate intake on insulin sensitivity, bodyweight, hemoglobin A1c, and blood pressure in patients with type 2 diabetes. J Am Diet Assoc; 105(4): 573-580.
“RESULTS: Both the high-carbohydrate and high-protein groups lost weight (-2.2+/-0.9 kg, -2.5+/-1.6 kg, respectively, P <.05) and the difference between the groups was not significant (P =.9). In the high-carbohydrate group, hemoglobin A1c decreased (from 8.2% to 6.9%, P <.03), fasting plasma glucose decreased (from 8.8 to 7.2 mmol/L, P <.02), and insulin sensitivity increased (from 12.8 to 17.2 micromol/kg/min, P <.03).” (emphasis added)
Some key aspects of the study
- N=12 (9 women, 3 men)
- All participants have type 2 diabetes
- Duration: 8 weeks
- Diets: high-carbohydrate (HC) diet (55% carbohydrate, 15% protein, 30% fat) and the high-protein/low-carb (HP) diet (40% carbohydrate, 30% protein, 30% fat)
- Weight loss: HC = 4.84 lbs , HP = 5.5 lbs
- Again, eating a diet of 40 to 55% carbs did not inhibit fat loss and eating 55% of carbs improved A1c, so it clearly was not having a negative impact on blood sugar regulation
2006-Differences in glycaemic status do not predict weight loss in response to hypocaloric diets in obese patients. Clinical Nutrition; 25(1):117-22
“Ability to lose weight on a hypocaloric diet over a 3-month time period does not vary in obese patients as a function of glycaemic status”
Some key aspects of the study
- N=76
- Age: mean of 46.7
- BMI: mean of 34.6
2010-Does the presence of metabolic syndrome [MetS] influence weight loss in obese and overweight women? Metabolic Syndrome and Related Disorders; 8(2): 173-178
“Conclusions: Obese and overweight patients with metabolic syndrome showed a greater reduction of their body weight, compared to the patients without metabolic syndrome. The components of the metabolic syndrome present at baseline correlated positively with the percentage of the weight loss. Finally, the patients with the highest levels of HOMA-index [greater insulin resistance] at baseline lost significantly more weight than those with lower levels of this parameter.”
Some key aspects of the study
- N=107 women
- Age: mean of 49.1
- BMI: mean of 35
- 3 month intervention
- Diet- a specific calorie amount was given to each person, overall goal of a daily 1,000 calorie deficit, calorie intake ranged from 1,085 to 2,000/day and was a low-fat diet, with macronutrient percentages being about 52% carbs, 28.5% fats and 19% protein
- Weight loss – no MetS = 9.9 lbs, with MetS = 56 lbs
- So having insulin resistance and eating a high carb diet did not inhibit weight loss
2010-One-year effectiveness of two hypocaloric diets with different protein/carbohydrate ratios in weight loss and insulin resistance. Nutr Hosp; 27(6):2093-2101
“The hypocaloric diets with different protein/carbohydrate ratios produced similar changes in weight…The present study…supports the theory that the macronutrient composition of a diet does not influence weight loss, body composition or improvements in insulin resistance.”
Some key aspects of the study
- N=40 (25 insulin resistant/IR)
- Gender: 27 female/13 male
- BMI: range of 28 to 35
- Age: range of 18 to 70, with a mean of 41.46
- Diet: 1,000 calorie deficit of estimated needs, with 2 different diets
- A-40% carbs, 30% protein, and 30% fat
- B-55% carbs, 15% protein, and 30% fat
- Duration: 12 months, but largest amount of weight loss was achieved at 6 months
- Weight loss: at 6 months, the authors state “no significant differences in weight loss percentages were found between IR and IS at 6 months”
- those with IR with diet A -10.25% or about 20 lbs, diet B -10.53% or about 20lbs
- those withoutIR (IS), with diet A -12.4% or about 23 lbs diet B -9.63% or about 18 lbs
- they did find that the group following the lower carb diet (40%) had better weight loss at 12 months, but this was still less than the amount at 6 months, which is not surprising as the evidence is clear that sticking to a diet is challenging. Again, eating a diet of 40% or 55% carbs did not inhibit fat loss
2015-Comparison of low and high carbohydrate diet for type 2 diabetes management: a randomized trial. Am J Clin Nutr; 102(4): 780-790
“Results: Both groups achieved similar completion rates…and mean (95% CI reductions in weight…blood pressure…HbA1c…fasting glucose…and LDL cholesterol”
Some key aspects of the study
- N=115
- BMI: 34.6
- Age: 58.7
- Gender: female =49, male =66
- All participants have type 2 diabetes, with a mean HbA1c of 7.3
- Duration: 52 weeks
- Diets: both hypocaloric, and matched for calorie intake
- Low carb (LC) 14% carbohydrate(carbohydrate <50 g/d), 28% protein, and 58% fat (<10% saturated fat)]
- High Carb (HC) was 53% carbohydrate, 17% protein, and 30% fat (<10% saturated fat
- Weight loss: LC mean of 20.68 lbs and HC mean of 22.22 lbs
- Eating carbs did not inhibit weight loss and actually resulted in slightly greater weight loss
2015-Effects of carbohydrate quantity and glycemic index [GI] on resting metabolic rate and body composition during weight loss. Obesity; 23(11): 2190-2198
“Conclusion-Moderate carbohydrate and low-GI diets did not preferentially reduce fat mass, preserve lean mass, or attenuate metabolic adaptation during weigh loss compared to high carbohydrate and high-GI diets”
Some key aspects of the study
- N=91 (79 completed all three phases)
- BMI: range 28-38
- Age: range of 45 to 65
- Gender: 39 male, 40 female
- Diet- four provided for diets, all are high carb, 55% or 70% and low-GI and highGI, all diets were matched for protein (16%)
- Duration: 17 weeks
- Weight loss: overall an average of 7.5% for all groups
- Eating high amounts of carbs did not inhibit weight loss
Two final papers before wrapping it up.
First is a very recent meta-analysis of 32 high quality randomized controlled feeding studies with isocaloric substitution of carbohydrate for fat.
2017-Obesity energetics: body weight regulation and the effects of diet composition. Gastroenterology; 152(7): 1718-1727.
The following is the summary chart from page 15, which gives a good visual of the different effects of low and high carb diets on weight loss.
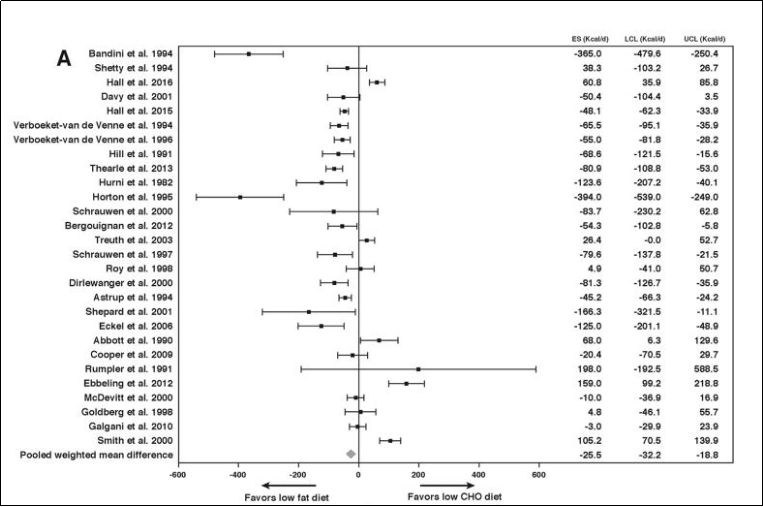
The authors conclude, “…our meta-analysis of 32 controlled feeding studies with isocaloric substitution of carbohydrate for fat found that both energy expenditure (26 kcal/d; P <.0001) and fat loss (16 g/d; P <.0001) were greater with lower fat diets.”
To be clear, the difference in fat loss is very small and is not clinically significant. However, the key take-away from this meta-analysis is the fact that low and high carb diets have almost the same weight loss benefits and high carbs diets do not inhibit fat loss.
Second, and finally, is a recent, large, high-quality study that looked at this question. Here are the details. It was an extensive study, so a bit more quoting and details are highlighted.
2017-Effect of low-fat vs low-carbohydrate diet on 12-month weight loss in overweight adults and the association with genotype pattern or insulin secretion: The DIETFITS randomized clinical trial. JAMA: 319(7): 667-679
“Question
What is the effect of a healthy low-fat (HLF) diet vs a healthy low-carbohydrate (HLC) diet on weight change at 12 months and are these effects related to genotype pattern or insulin secretion?
Findings
In this randomized clinical trial among 609 overweight adults, weight change over 12 months was not significantly different for participants in the HLF diet group (−5.3 kg) vs the HLC diet group (−6.0 kg), and there was no significant diet-genotype interaction or diet-insulin interaction with 12-month weight loss.
Meaning
There was no significant difference in 12-month weight loss between the HLF and HLC diets, and neither genotype pattern nor baseline insulin secretion was associated with the dietary effects on weight loss.”
Some key aspects of the study
- N=609
- BMI: mean of 33
- Age: mean of 40
- Gender: 263 males, 346 women
- Duration:12 months
- Diets: 2 groups, low fat and low carb, for both there was no recommendation to reduce overall calorie intake (was ad libitum),
- Here is the protocol from the paper:
“Briefly, the main goals were to achieve maximal differentiation in intake of fats and carbohydrates between the 2 diet groups while otherwise maintaining equal treatment intensity and an emphasis on high-quality foods and beverages. Thus, participants were instructed to reduce intake of total fat or digestible carbohydrates to 20 g/d during the first 8 weeks. Higher priorities for reduction were given to specific foods and food groups that derived their energy content primarily from fats or carbohydrates. For example, the reduction of edible oils, fatty meats, whole-fat dairy, and nuts was prioritized for the healthy low-fat group, whereas the reduction of cereals, grains, rice, starchy vegetables, and legumes was prioritized for the healthy low-carbohydrate group.
Then individuals slowly added fats or carbohydrates back to their diets in increments of 5 to 15 g/d per week until they reached the lowest level of intake they believed could be maintained indefinitely. No explicit instructions for energy (kilocalories) restriction were given. Both diet groups were instructed to (1) maximize vegetable intake; (2) minimize intake of added sugars, refined flours, and trans fats; and (3) focus on whole foods that were minimally processed, nutrient dense, and prepared at home whenever possible. Other components of the emphasis on high-quality food for both diet groups are described elsewhere.” (emphasis added)

- From Table 2, you can see there was a clinically significant difference in carb intake between the 2 groups. It was even more significant the first couple of months. But the overall differences of carb intake at the end of the 12 months was;
- 4%/212.9g for LF vs 29.8%/132g for LC.
- Weight loss (mean): LF=11.6 lbs, LC=13.2 lbs
This large, long-term, high-quality study showed again; carb intake and different insulin responses do not inhibit fat loss.
Before concluding I want to make it clear, low carb eating is ONE possible good option. For some people in certain situations, low-carb, including keto (although these can have different effects as well), may have some additional positive metabolic effects (ie., BP, blood sugar, triglycerides, etc) when compared to higher carb diets during weight maintenance (eucaloric state). During weight loss (hypocaloric state), however, there are no advantages to either low or high carb diets, since calorie restriction and subsequent fat loss seems to produce all or most of the metabolic benefits, regardless of macronutrient amounts and even the quality of the diet. Additionally, low carb diets do not produce more fat loss and they are not automatically easier to follow than a higher carb diets.
Conclusion
Insulin and carbs are not the boogeymen they can be portrayed as (by many low carb/keto people). A convergence of evidence over many decades, particularly the past 20 years, has clearly shown that calories is the number one factor that determines fat loss (and fat gain, btw). How people can be consistent with creating a calorie deficit, which can be difficult, can vary widely, and a wide range of macronutrient intakes as well as meal frequency (to name a couple major variables) can influence this. Furthermore, it does not have to be one eating plan forever. There is nothing wrong with changing things up. This could be needed due to changes in life circumstances or just for the sake of doing something different which can have psychological advantages. Feeling like there is only “one” way to lose weight can have many negative effects on psychological variables such as motivation and adherence. When it comes to fat loss, the only real “magic” to any eating plan is if it helps a person consistently eat the number of calories that elicits a pace of weight loss they want. At the end of the day, when it comes to losing fat, it’s about consistency.
For those interested the following are some other insightful articles on this topic
Hall, K. (2017). A review of the carbohydrate-insulin model of obesity. European J Clinical Nutrition
Aragon et al (2017) International society of sports nutrition position stand: diets and body composition. Journal of the International Society of Sports Nutrition; 14:16
https://weightology.net/insulin-an-undeserved-bad-reputation/
http://carbsanity.blogspot.com/2018/12/the-12m-nusiludwig-study-part-iv.html
https://examine.com/nutrition/low-fat-vs-low-carb-for-weight-loss/
http://sciencedrivennutrition.com/do-carbohydrates-control-body-fat/
http://sciencedrivennutrition.com/body-weight/
http://sciencedrivennutrition.com/nail-low-carb-coffin/